fetching data ... 
Background: Physical activity (PA) is a key non-pharmacological component of management in patients with axial spondyloarthritis (axSpA). In routine clinical practice, PA is most often assessed using self-reported questionnaires, which may not accurately reflect real-life movement. Objective assessment using step count represents a simple and scalable approach; however, the clinical relevance of discordance between perceived and objectively measured PA in axSpA remains insufficiently explored.
Objectives: To assess physical activity in patients with axSpA using both self-reported and objectively measured parameters, to quantify discordance between these measures, and to identify clinical, functional, and psychosocial characteristics associated with discrepant PA phenotypes.
Methods: This cross-sectional study included 63 patients with axSpA, all in remission or low disease activity at the time of assessment. Self-reported PA was assessed using the International Physical Activity Questionnaire (IPAQ). Objective PA was assessed using digitally recorded daily step count over seven consecutive days. A threshold of 7,000 steps/day was applied [1]. Fatigue was assessed using the Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F), depressive symptoms using the Patient Health Questionnaire-9 (PHQ-9), kinesiophobia using the Tampa Scale, and sarcopenia risk using the SARC-F questionnaire. Demographic characteristics, disease duration, treatment characteristics, and the presence of peripheral and extra-articular manifestations were obtained from electronic records. Patients reporting moderate-to-high PA by IPAQ were further stratified according to objectively measured step count into two phenotypes: low steps/high IPAQ (discordant phenotype) and high steps/high IPAQ (concordant phenotype). Group comparisons were performed using non-parametric tests. Categorical variables were analyzed using Fisher’s exact test. Multivariable logistic regression analysis was applied to identify independent predictors of the discordant phenotype.
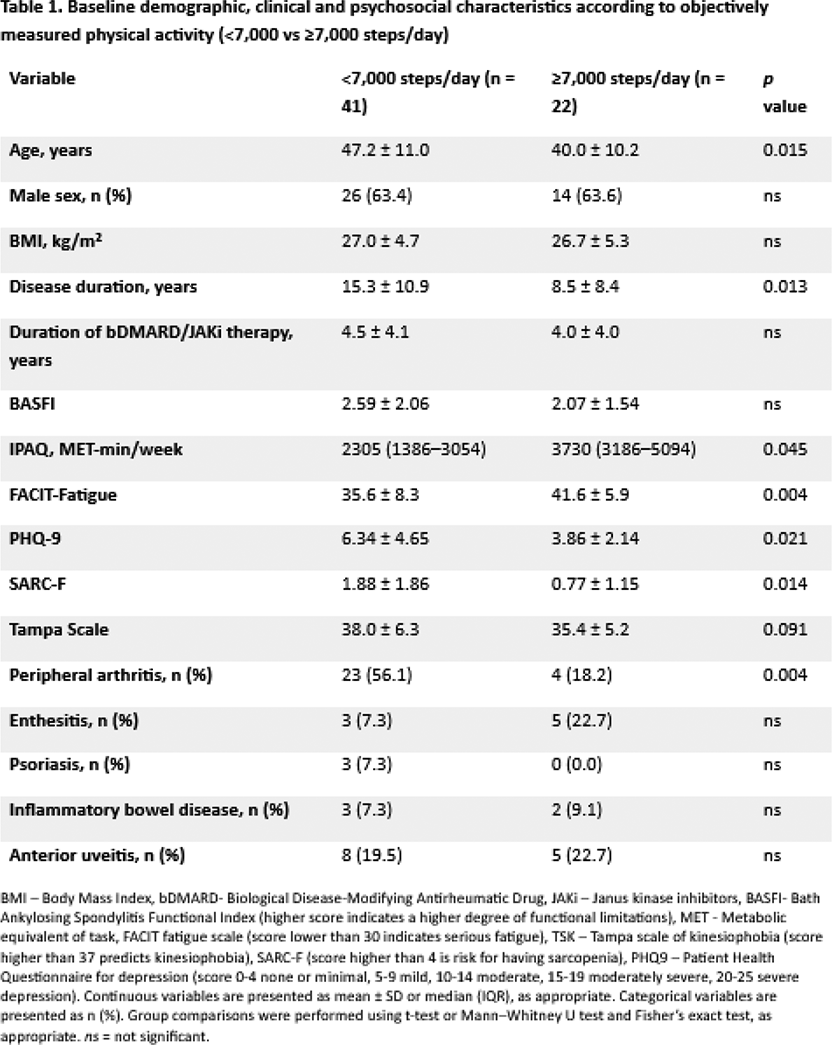
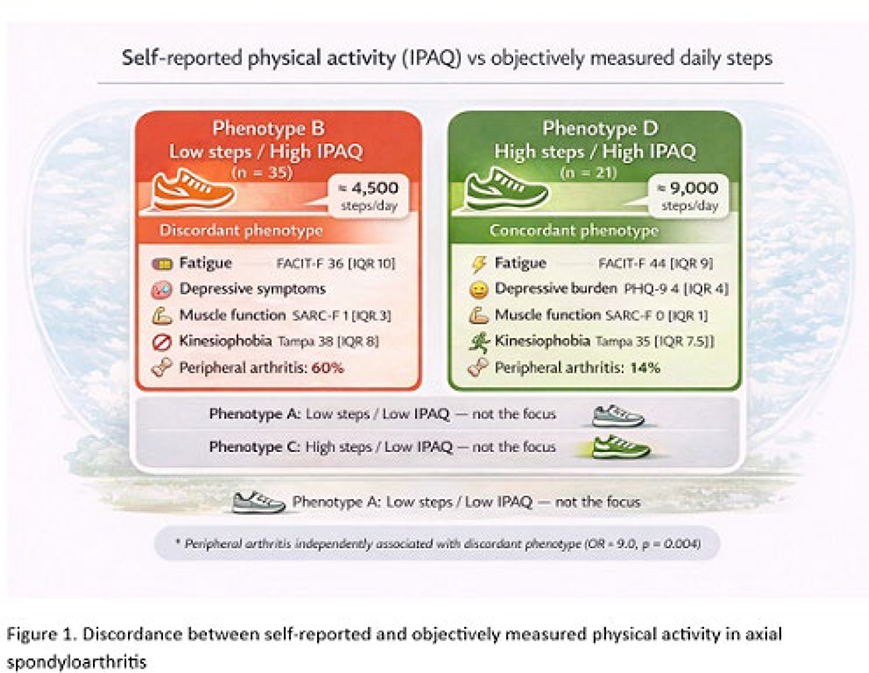
Results: The study population comprised 40 (63.5%) male and 23 (36.5%) female patients, with a median age of 46 years (IQR 37–53). The median objectively measured daily step count was 5,924 steps/day (IQR 4,138–8,112). Based on the 7,000 steps/day threshold, 41 patients (65.1%) were classified as having low objective physical activity. Patients with <7,000 steps/day were older and had longer disease duration, and demonstrated higher fatigue, greater depressive symptom burden, worse muscle function, and higher levels of kinesiophobia compared with those achieving ≥7,000 steps/day (all p < 0.05), while no differences were observed in sex distribution, body mass index, treatment characteristics, or functional status (Table 1). According to IPAQ classification, 7 patients (11.1%) reported low physical activity, while 36 (57.1%) and 20 (31.7%) reported moderate and high physical activity levels, respectively. Despite predominantly moderate-to-high self-reported physical activity by IPAQ, 35 of 56 patients (62.5%) failed to achieve ≥7000 steps/day. Compared with concordantly active patients, the discordant phenotype (low steps/high IPAQ) was characterized by older age, longer disease duration, higher fatigue, depressive symptoms, impaired muscle function, and increased kinesiophobia (all p < 0.05). Peripheral arthritis was significantly more prevalent in the discordant phenotype (60.0% vs 14.3%, p = 0.001) and remained independently associated with this phenotype after adjustment for age and disease duration (OR ≈ 9.0, p = 0.004) (Figure 1). No differences were observed between phenotypes regarding educational level, marital or employment status, disability status, smoking, comorbidities, or the presence of extra-articular manifestations, including enthesitis, psoriasis, inflammatory bowel disease, or uveitis.
Conclusions: Despite controlled inflammatory disease activity, a substantial proportion of patients demonstrated discordance between perceived and objectively measured physical activity. The association with a history of peripheral arthritis and higher levels of kinesiophobia suggests that behavioral and psychosocial factors may persist beyond inflammatory control and continue to limit real-life movement in axial spondyloarthritis. These findings highlight the need for objective assessment of physical activity and for multidisciplinary strategies addressing movement-related fear and long-term functional behavior, in addition to optimal pharmacological disease control.
REFERENCES: [1] Ding D. Daily steps and health outcomes in adults: a systematic review and dose-response meta-analysis. Lancet Public Health. 2025 Sep;10(9):e731. doi: 10.1016/S2468-2667(25)00199-9.
Acknowledgments: NIL.
Disclosure of Interests: None declared.