fetching data ... 
Background: Patient partnership in the design and conduct of clinical research is increasingly seen as best practice, particularly so for the development of a clinical outcome assessment (COA) intended for use in clinical trials supporting drug registration. Patient-Focused Drug Development (PFDD) mandates that a COA must be able to detect meaningful changes in how a patient feels, functions or survives [1]. To address the need for improved COAs for Systemic Lupus Erythematosus (SLE) clinical trials, an international Taskforce has developed the novel Treatment Response Measure for Systemic Lupus Erythematosus (TRM-SLE) COA. Patients were major contributors to this work.
Objectives: To describe the involvement of patients and patient organisation representatives in TRM-SLE COA development and report patient perspectives on their involvement in the project.
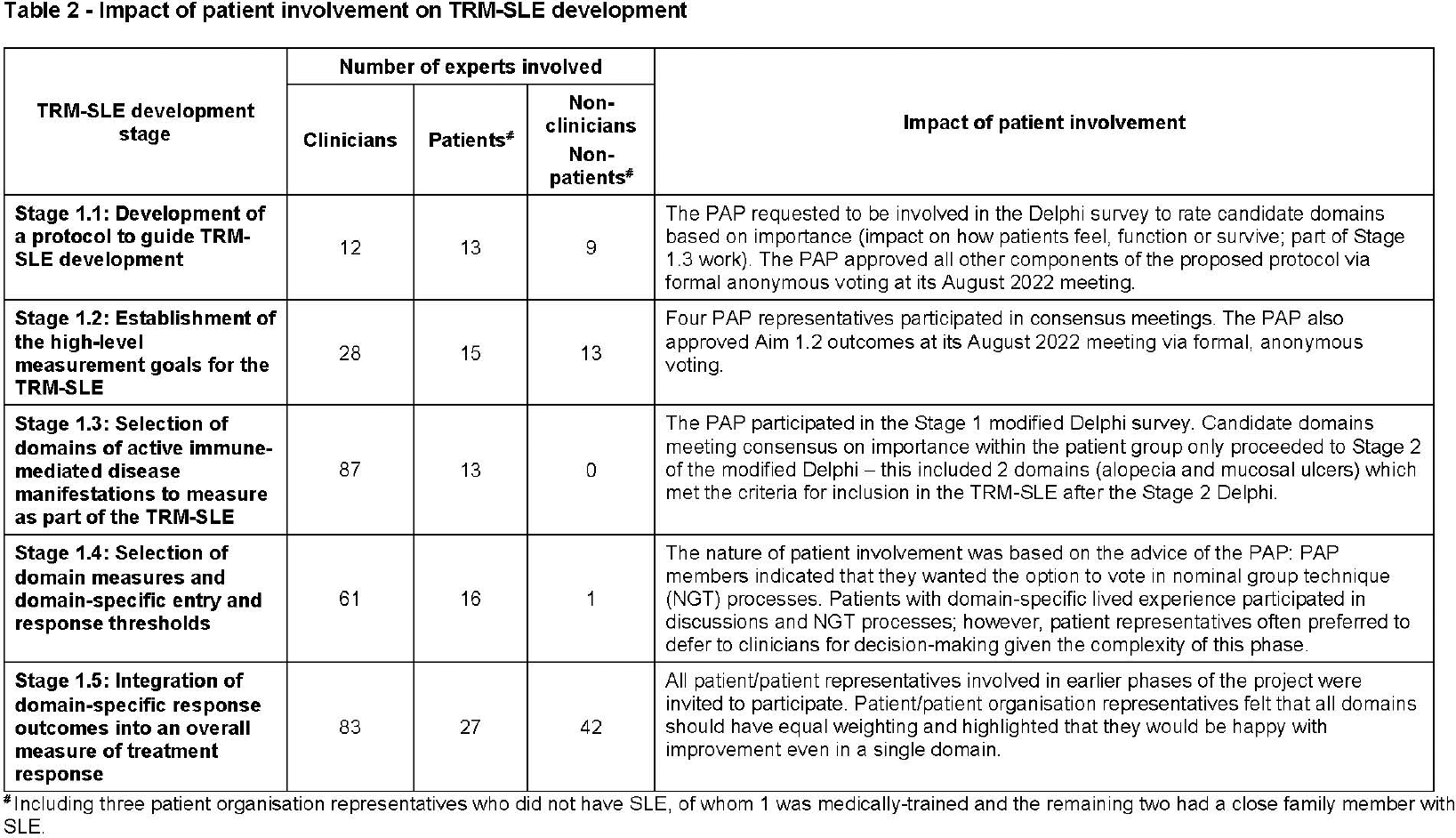
Methods: Development of the TRM-SLE involved expert consensus processes (Delphi and nominal group techniques) to (i) develop a protocol to guide development of the TRM-SLE (ii) establish the high-level measurement goals for TRM-SLE (iii) select domains of active immune-mediated disease manifestations to measure as part of TRM-SLE (iv) select domain measures and domain-specific entry and response thresholds and (v) integrate domain-specific response outcomes into an overall measure of treatment response [2]. Consensus outcomes and meeting proceedings were reviewed to assess the impact of patient involvement in the project. Additionally, patient perspectives on their involvement in the project were also captured.
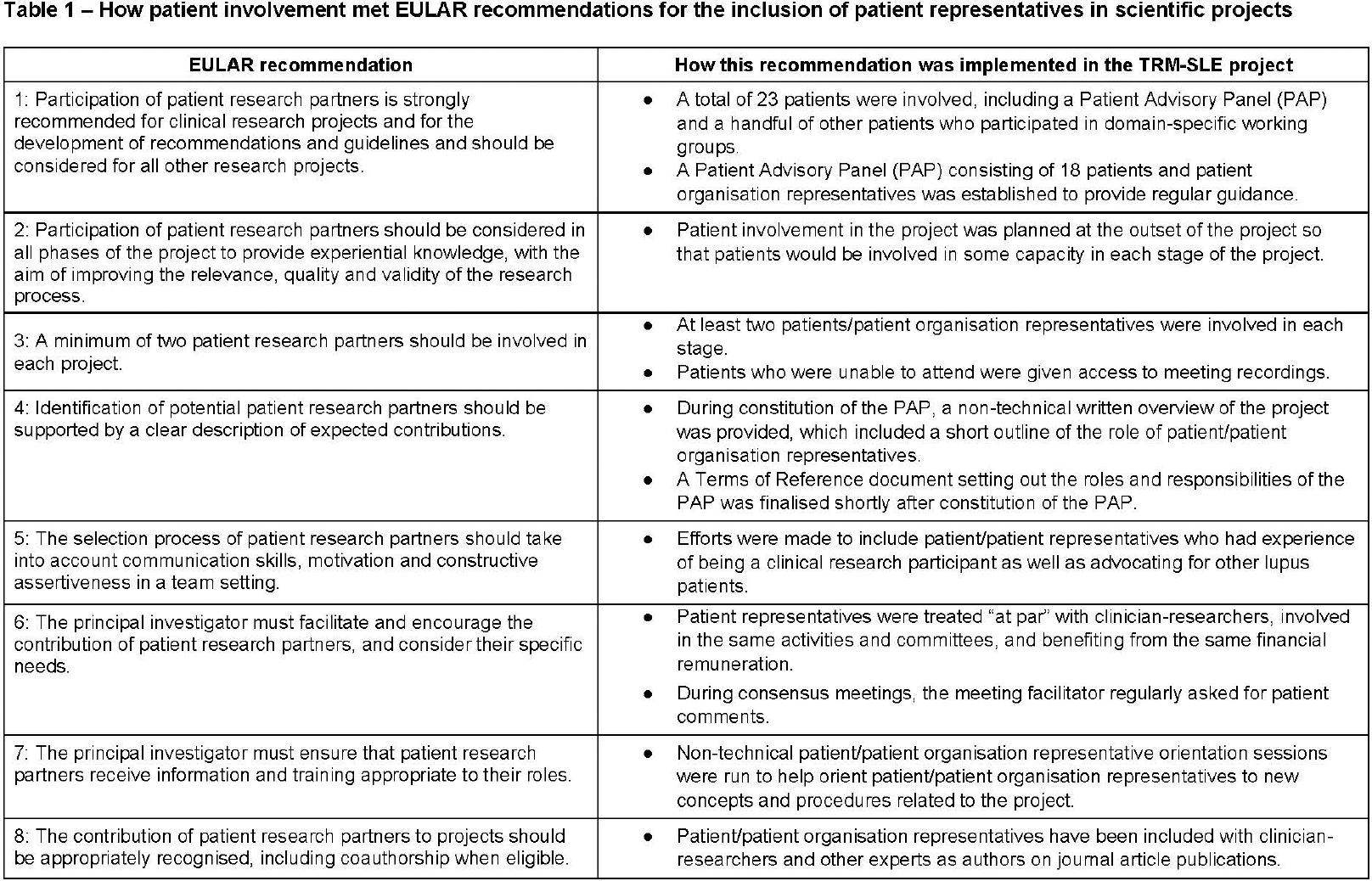
Results: In line with European Alliance of Associations for Rheumatology (EULAR) recommendations [3], patient/patient organisation representatives were involved in all phases of the project (see Table 1 for further details). To facilitate this, a Patient Advisory Panel (PAP) was established early in the project. Patient representatives were provided with an outline of their role in the project, specifically to provide guidance regarding the patient experience of lupus in relation to important elements to include in a COA for use in SLE trials, but provided input regarding how they could best be involved in the project. Non-technical orientation sessions were provided to introduce new concepts and processes. Notably, patient representatives were treated “at par” with clinician-researchers, involved in the same activities and committees, and benefiting from the same financial remuneration. This led to significant changes, particularly during the domain selection process, where patient input led to inclusion of domains that were not considered as important by clinicians (Table 2). Patients reported a positive experience of being involved in the project and described the patient involvement to be “real” and for their input to be given full consideration: “that domain of living with a disease was listened to as much as the domain of knowing scientifically the disease.” Access to meeting recordings was discussed by several patient representatives as assisting with patient involvement: “So, you might be able to join the meeting and listen in... sometimes it just went over our head. But we were able to listen to it again, look into the data, look some things up and then it made sense. And also sometimes if you don’t feel well enough to join the meetings and we still could listen to the meetings afterwards.”
Conclusions: Patient participation alongside clinician-researchers in clinical research and PFDD is not only achievable when planned at the outset but also contributes to a better outcome of the project. It is important that patients feel comfortable to share their perspective and to orient patient/patient organisation representatives to technical concepts to maximise their participation.
REFERENCES: [1] US Department of Health and Human Services Food and Drug Administration, 2022. Patient-Focused Drug Development Guidance Series for Enhancing the Incorporation of the Patient’s Voice in Medical Product Development and Regulatory Decision Making. Selecting, Developing, or Modifying Fit-for-Purpose Clinical Outcome Assessments (Draft Guidance).
[2] Connelly, K., Eades, L., Koelmeyer, R. et al., 2023. Towards a Novel Clinical Outcome Assessment for Systemic Lupus Erythematosus: First Outcomes of an International Taskforce. Nature Reviews Rheumatology; 19(9): p. 592-602.
[3] de Wit, M. P. T., Berlo, S. E., Aanerud, G. J. et al., 2011. European League Against Rheumatism recommendations for the inclusion of patient representatives in scientific projects. Ann Rheum Dis ; 70: 722-726.
Acknowledgments: NIL.
Disclosure of Interests: Rachel Koelmeyer: None declared, Alain Cornet: None declared, Amy Somers: None declared, Annemarie Sluijmers: None declared, Blanca Rubio: None declared, Cathrine Hjelmeset: None declared, Dalila Tremarias: None declared, Dalilah Kalla: None declared, Francesca Marchiori: None declared, Gonzalo Tobar: None declared, Imasha Adisa: None declared, Judith Mills: None declared, Khadija Dantata: None declared, Narae Yun: None declared, Shiori Nagamori: None declared, Sibongile Komati: None declared, Najha Black: None declared, Stephanie Scoggins: None declared, Susanne Gydesen: None declared, Toni Grimes: None declared, Vinita Haroun: None declared, Zoe Karakikla Mitsakou: None declared, Kathryn Connelly AstraZeneca, Eric Morand AstraZeneca, Merck Serono and Novartis, AbbVie, AstraZeneca, Biogen, Bristol Myers Squibb, Galapagos, Gilead, Genentech-Hoffman La Roche, GlaxoSmithKline, EMD Serono, Janssen, Merck, Novartis, Quell, Remegen, UCB and Zenas, AbbVie, Amgen, AstraZeneca, Biogen, Bristol-Myers Squibb, Eli Lilly, Genentech-Hoffman La Roche, GlaxoSmithKline, Janssen, Merck KGaA Darmstad Germany, Merck Serono, Novartis, Takeda, UCB and Union Chimique Belge, Darshini Ayton: None declared, Katie Liao: None declared, Joy Buie: None declared, Jeanette Andersen: None declared