fetching data ... 
Background: The waxing and waning nature of SLE makes it difficult to demonstrate efficacy of novel treatment in clinical trials. Many trials have failed due to enrollment of inappropriate patient populations, or patients in varying stages of disease activity.
Objectives: To quantify the prognostic value of pre-baseline SLE disease activity trends and early follow-up data for predicting 12 month disease activity outcomes.
Methods: We analyzed patients with SLE from the Toronto Lupus cohort (1) with baseline SLEDAI-2K ≥6 and a year of prior data treated with standard of care. Outcomes modeled included absolute and percentage change in SLEDAI-2K values and an SRI-4 response (≥4 point reduction) at 12 months. Predictors included demographics, laboratory and serologic markers, SLEDAI-2K at baseline and its 1 year pre-baseline trajectory (average slope and range), baseline treatments, and 3 month interim SLEDAI-2K. We trained regression and machine learning models on four predictor sets: baseline SLEDAI-2K alone; full baseline covariates (with pre-baseline trajectory); baseline SLEDAI-2K with 3 month interim data; and full baseline covariates with interim data. Model performance was assessed via cross validation (R 2 for numerical outcomes, ROC AUC for SRI-4). We also assessed the contribution of the pre-baseline SLEDAI-2K slope and model performance reduction when removing it from the model.
Results: Among 337 patients (median baseline SLEDAI-2K 8.0, disease duration 12.3 years, pre-baseline slope 3.2 points/year), 77% had reduced SLEDAI-2K at 12 months (median –3.8 points, –40.8%) and 61% achieved SRI-4 response.
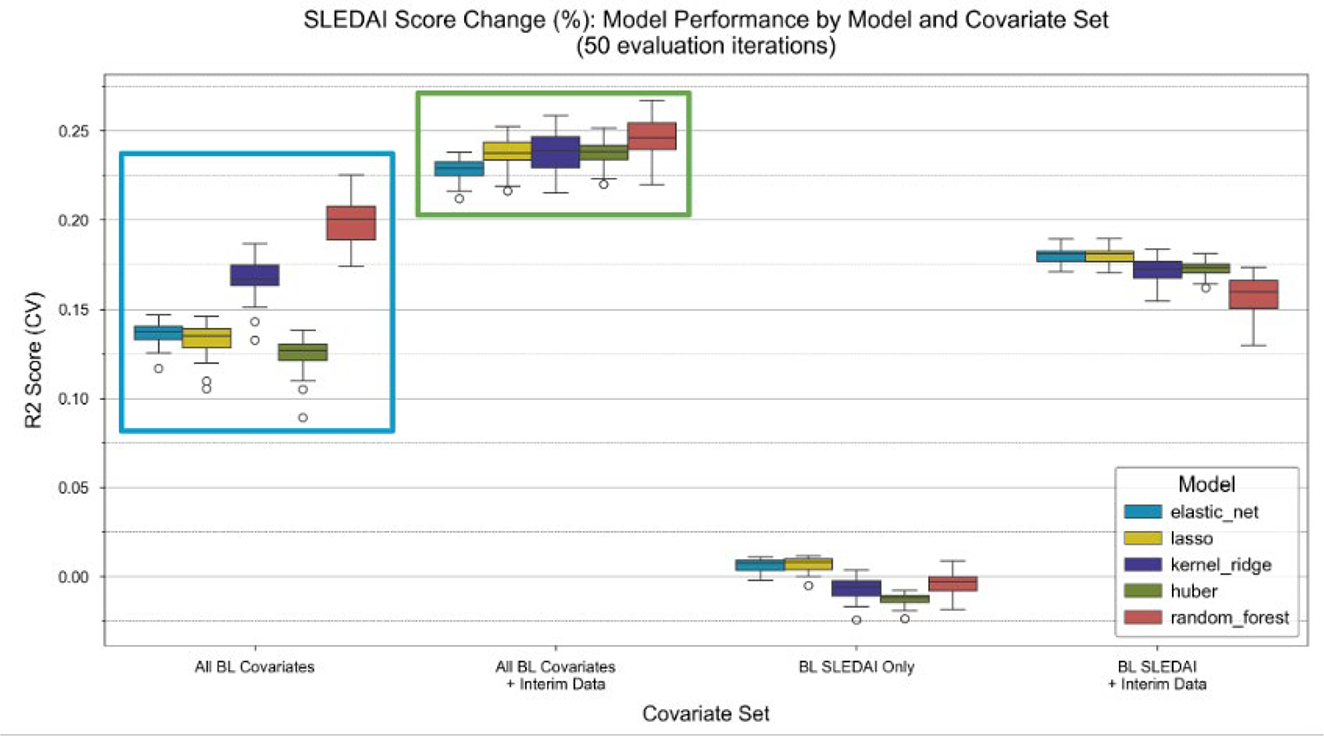
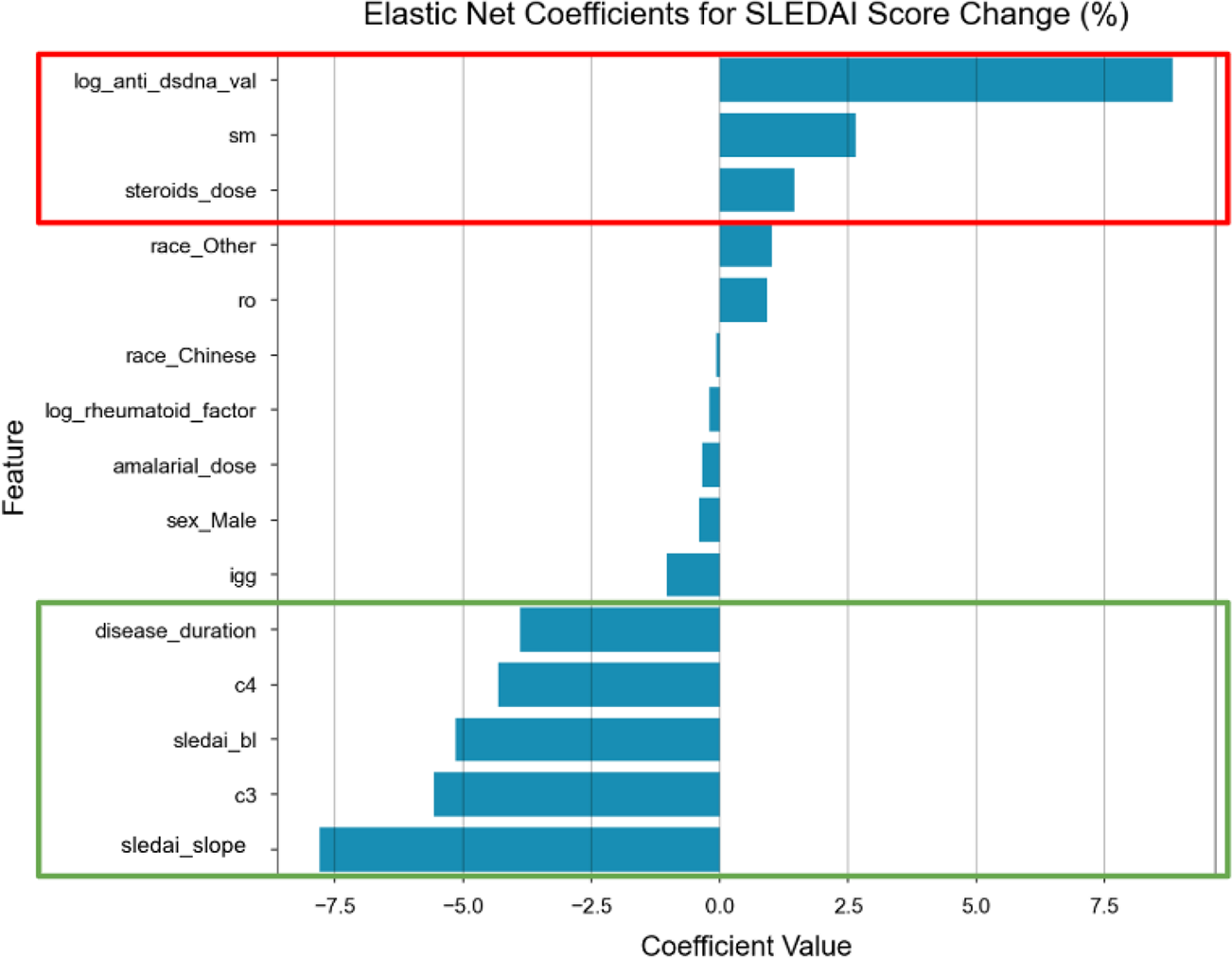
Models with full baseline covariates outperformed those with baseline SLEDAI-2K alone, especially for percentage change (R 2 improving from ~0 to 0.13–0.20, and to 0.23–0.25 with interim data) (figure 1). Notably, a worsening pre-baseline SLEDAI-2K slope was associated with better outcomes in disease activity. This persisted with inclusion of 3 month interim treatment data, suggesting that treatment intensification alone does not fully explain the effect. The pre-baseline SLEDAI-2K slope remained significantly predictive of SRI-4 response (OR ~1.98, p<0.001) when adjusting for baseline disease activity, indicating independent prognostic value beyond baseline severity. Removing the slope reduced model performance, particularly for percentage change. Known serologic and therapy factors (anti-dsDNA, anti-Smith, high corticosteroids, low complement) predicted worse outcomes in disease activity (figure 2).
Conclusions: The 1 year pre-baseline SLEDAI-2K slope and 3 month interim data capture disease dynamics that improve prediction of 12 month outcomes beyond patients’ baseline characteristics. A worsening disease activity trajectory prior to baseline was associated with better outcomes, suggesting effects of treatment escalation or regression to the mean. Accounting for disease activity trajectory in clinical trial design could modify inclusion criteria and support adaptive designs for ongoing studies. These data may also enhance the interpretability and validity of prognostic models and disease activity outcome assessments.
Performance of Prediction Models Across different variables (Covariate Sets) for 12-Month SLEDAI-2K Total Score Change (%). Models using the full set of baseline covariates outperform those using only the baseline SLEDAI-2K score. Performance improves further with the addition of 3-month interim data.
Key features Predicting SLEDAI-2K Total Score Change (%) as Identified by a Linear Regression Model (Regularized). Key predictors of negative outcomes (red) include anti-dsDNA, corticosteroid dose. While key predictors of positive outcomes (green) include high complement as well as baseline SLEDAI-2K and its 1-year pre-baseline slope. This shows that the disease activity trajectory before baseline helps predict outcomes. In particular, patients with a worsening trajectory prior to baseline tended to improve more over 12 months.
REFERENCES: [1] Tselios K, Gladman DD, Su J, Ace O, Urowitz MB. Evolution of Risk Factors for Atherosclerotic Cardiovascular Events in Systemic Lupus Erythematosus: A Longterm Prospective Study. J Rheumatol. 2017 Dec;44(12):1841-1849. doi: 10.3899/jrheum.161121. Epub 2017 Nov 1. PMID: 29093154.
Acknowledgments: NIL.
Disclosure of Interests: None declared.