fetching data ... 
Background: The management of systemic lupus erythematosus (SLE) varies worldwide. Current SLE treatment goals focus on preventing flares, controlling disease activity, and preventing organ damage accrual. LupusNet is the largest federated data network in SLE that combines and harmonizes data from 5 existing registries to enable greater data consistency and enhance understanding of global clinical presentations and outcomes of SLE.
Objectives: This study assessed treatment patterns for patients with SLE, categorized by disease severity, from LupusNet and a US claims database.
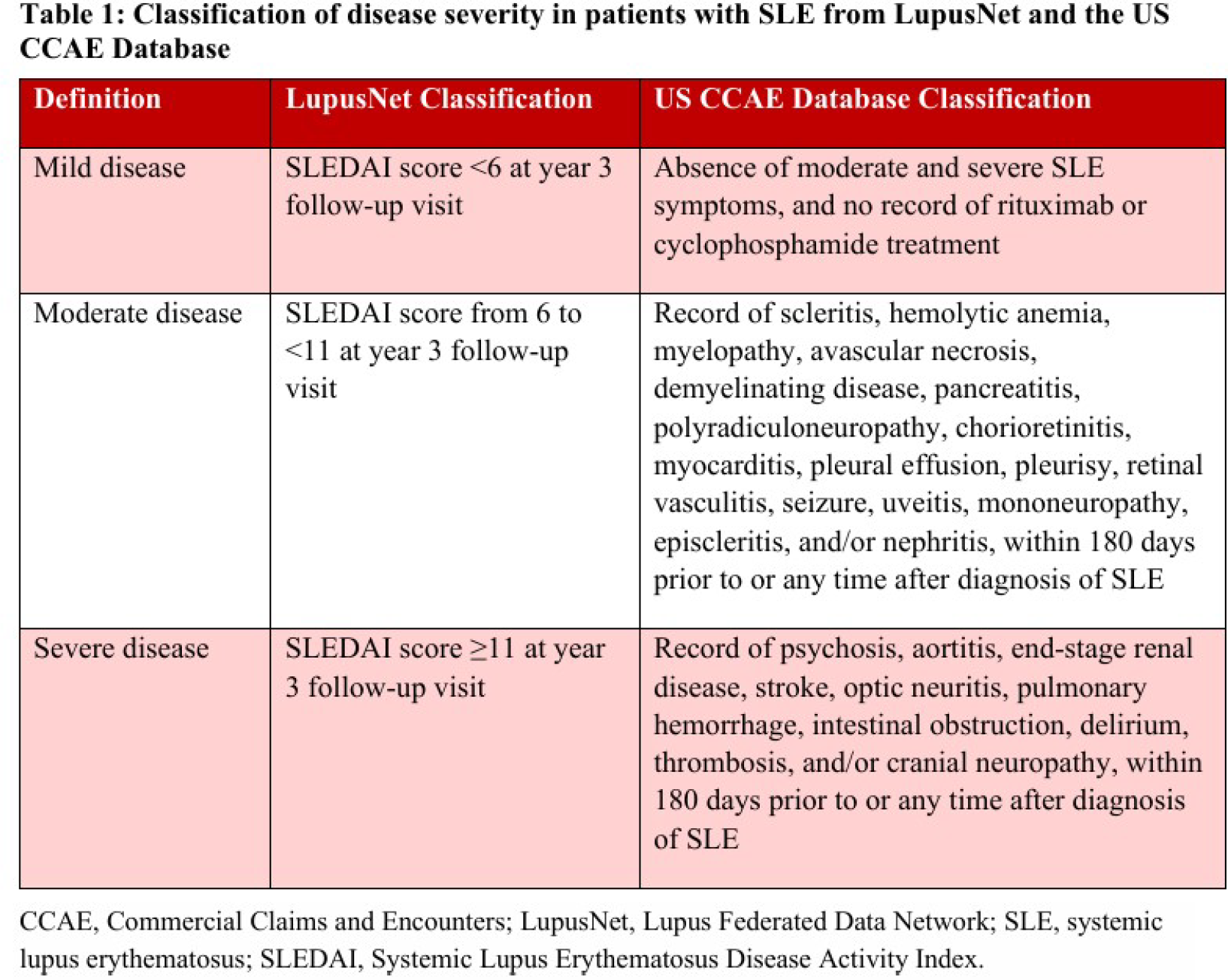
Methods: Data from 3 of 5 SLE registries in LupusNet, APLC (Asia Pacific), RELESSER (Europe), and Almenara (South America), were analyzed from 2012 to 2024, using a privacy-preserving federated data network approach, where only aggregated results were shared. Additionally, data from the US Merative MarketScan ® Commercial Claims and Encounters (CCAE) Database from 2019 to 2024 were included in the analysis. In LupusNet, data from patients with ≥3 years of follow-up and ≥3 follow-up visits were collected and stratified into mild, moderate, or severe disease based on a SLEDAI score at year 3 follow-up visit ( Table 1 ). In the US claims database, data from patients who were diagnosed with SLE were stratified by mild, moderate, or severe disease based on documented symptoms and clinical features ( Table 1 ). Treatment exposures (i.e., glucocorticoids, antimalarials, immunosuppressants, biologic therapies, and other immunosuppressants/immunomodulators) were assessed over follow-up.
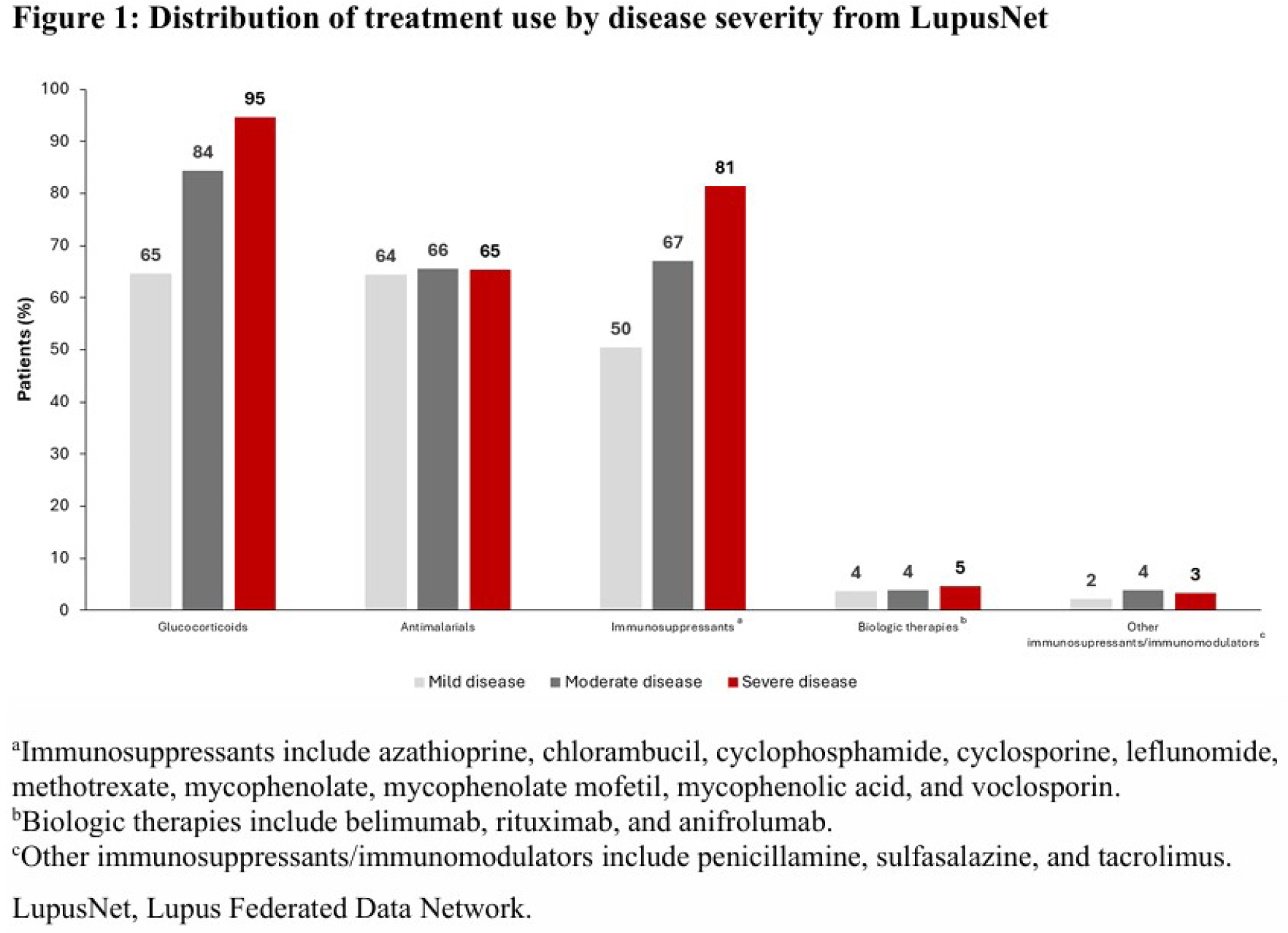
Results: LupusNet included 3857 eligible patients: 3070 with mild disease, 637 with moderate disease, and 150 with severe disease. US claims data included 49,350 eligible patients: 23,461 with mild disease, 16,172 with moderate disease, and 9717 with severe disease. Glucocorticoid use was widespread across all disease severity levels: 63%-65% of patients with mild disease, 76%-84% with moderate disease, and 89%-95% with severe disease received glucocorticoids in both the LupusNet and US claims data ( Figure 1 ). Antimalarials were also frequently prescribed in 58%-66% of patients, regardless of disease severity. In contrast, use of immunosuppressants varied with disease severity: 25%-50% of patients with mild disease, 43%-67% with moderate disease, and 69%-81% with severe disease received immunosuppressants. Biologic therapies and other immunosuppressants/immunomodulators were utilized less frequently across all disease severity levels in LupusNet (4% and 2%-4%, respectively), while the use of these therapies increased with disease severity in US claims data (8%-44% and 4%-13%, respectively).
Conclusions: This analysis of patient data from LupusNet registries and the US claims database revealed that a considerable number of patients with active, severe SLE across geographic locations were not receiving immunosuppressants or biologic therapies. This suggests a heavy dependence on glucocorticoids to control disease activity and a potential underutilization of steroid-sparing therapies. Additional research is needed to explore long-term treatment trends and barriers to accessing treatments in patients with SLE.
REFERENCES: NIL.
Acknowledgments: NIL.
Disclosure of Interests: Ashley Orillion Johnson & Johnson, Johnson & Johnson, Federico Zazzetti Johnson & Johnson, Johnson & Johnson, Anna Sheahan Johnson & Johnson, Johnson & Johnson, Clair Blacketer Johnson & Johnson, Johnson & Johnson, Michel van Speybroeck Johnson & Johnson, Johnson & Johnson, Sarah Gasman Johnson & Johnson, Johnson & Johnson, Reyhan Sonmez Johnson & Johnson, Johnson & Johnson, Erika Noss Johnson & Johnson, Johnson & Johnson, Manuel F. Ugarte-Gil AstraZeneca, Ferrer, GSK, Novartis, and Tecnofarma, AstraZeneca, Ferrer, GSK, Novartis, and Tecnofarma, Johnson & Johnson, Rocío V. Gamboa-Cárdenas: None declared, Victor R. Pimentel-Quiroz: None declared, Kaleb Michaud: None declared, Patricia Katz: None declared, Rangi Kandane-Rathnayake BMS, GSK and Novartis, Eric Morand Dragonfly, Quell, Remegem, and Zenas, Dragonfly, Quell, Remegem, and Zenas, Abbvie, Amgen, AstraZeneca, Biogen, BMS, Eli Lilly, EMD Serono, Genentech, GSK, Johnson & Johnson, Novartis, Roche, Takeda, and UCB, Worawit Louthrenoo: None declared, Alberta Hoi AstraZeneca, BMS, Eli Lilly, and UCD; advisor or review panel member for GSK and Johnson & Johnson; and provided contract research to Merck/MSD, Yi-Hsing Chen Pfizer, Novartis, Abbvie, Johnson & Johnson, BMS, Roche, Lilly, GSK, AstraZeneca, Sanofi, MSD, Guigai, Astellas, Inova Diagnostics, UCB, Agnitio Science Technology, United Biopharma, Thermo Fisher, Gilead, Eisai, CSL Behring, from Taiwan Ministry of Science and Technology, Taiwan Department of Health, Taichung Veterans General Hospital, GSK, BMS, AstraZeneca, Medigen Vaccine Biologics, Pfizer, Novartis, Abbvie, Johnson & Johnson, Roche, Sanofi, Guigai, Boehringer Ingelheim, UCB, MSD, Astellas, Gilead, Biogen, and Celldex, Jiacai Cho: None declared, Laniyati Hamijoyo: None declared, Shue Fen Luo: None declared, Sandra Navarra Astellas, AstraZeneca, Aurinia, Biogen, and Idorsia/Viatris, Astellas, AstraZeneca, Aurinia, Biogen, and Idorsia/Viatris, Mandana Nikpour AstraZeneca, Boehringer-Ingelheim, BMS, GSK, and Johnson & Johnson, AstraZeneca, Boehringer-Ingelheim, BMS, GSK, and Johnson & Johnson, José M. Pego-Reigosa AstraZeneca, GSK, and Otsuka, AstraZeneca and GSK, Íñigo Jesus Rúa-Figueroa: None declared, Zulema Plaza: None declared, Maria Galindo Izquierdo: None declared, Julia Martínez-Barrio: None declared, Jaime Calvo Alén: None declared, Antonio Fernández-Nebro AstraZeneca, Eli Lilly, Galapagos, Gebro Pharma, GSK, and Novartis, AstraZeneca, Eli Lilly, Galapagos, Gebro Pharma, GSK, and Novartis, Argenx, AstraZeneca, Chemo, Galapagos, Johnson & Johnson, Merck Serono, MSD, Novartis, Takeda, and UCB, Raúl Menor-Almagro: None declared, Eva Tomero Muriel: None declared, Francisco Javier Narváez Garcia: None declared, Chetan S. Karyekar Johnson & Johnson, Johnson & Johnson.