fetching data ... 
Background: Systemic lupus erythematosus (SLE) is a chronic autoimmune disease characterized by significant clinical heterogeneity and the potential to affect multiple organ systems [1]. Clinical observations indicate that cardiovascular involvement is a prevalent comorbidity in this patient population, associated with a mortality rate significantly higher than that of the general population [2]. The pathogenesis of these complications is primarily linked to an increased risk of thrombosis and accelerated atherosclerosis, notably marked by abnormal deposition of atherosclerotic plaques [3]. Understanding the mechanisms and risk factors of cardiovascular comorbidities in SLE patients is crucial to guide early risk identification, stratified management, and personalized care.
Objectives: This study aimed to compare the clinical, metabolic, and immunological profiles between SLE patients with and without cardiovascular disease (CVD), with a focus on Th1/Th2 imbalance and its association with cardiometabolic risk.
Methods: A total of 1,325 SLE patients followed at the Department of Rheumatology and Immunology, Second Hospital of Shanxi Medical University, were enrolled. Based on the presence of cardiovascular disease—defined as including coronary heart disease, heart failure, arrhythmia, and excluding isolated hypertension—patients were divided into two groups:SLE-CVD+ group and the SLE-CVD- group. Demographic data and clinical indicators were collected and compared between the two groups. The analysis of lymphocyte subgroups was conducted using flow cytometry, following standardized operating procedures to ensure accuracy and reproducibility.Statistical analyses were conducted using IBM SPSS software (version 27; IBM Corp, Armonk, New York, USA).Statistical significance was defined as P<0.05.
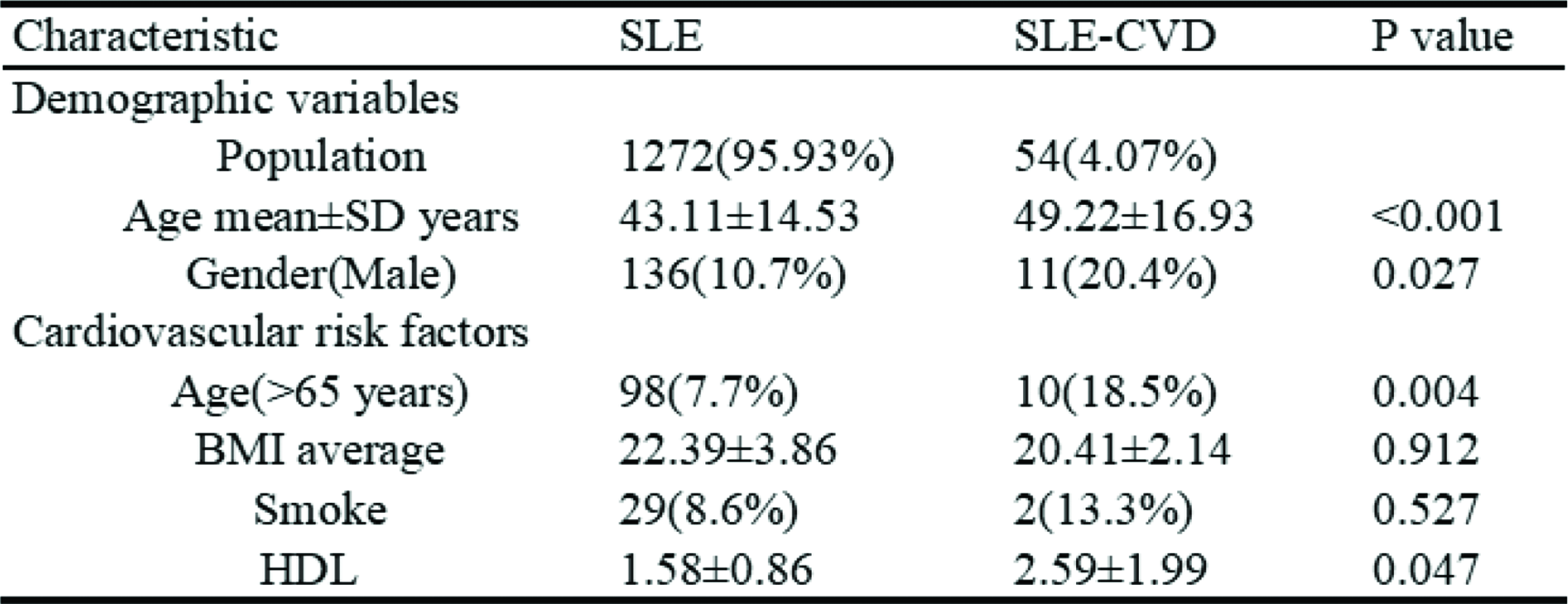
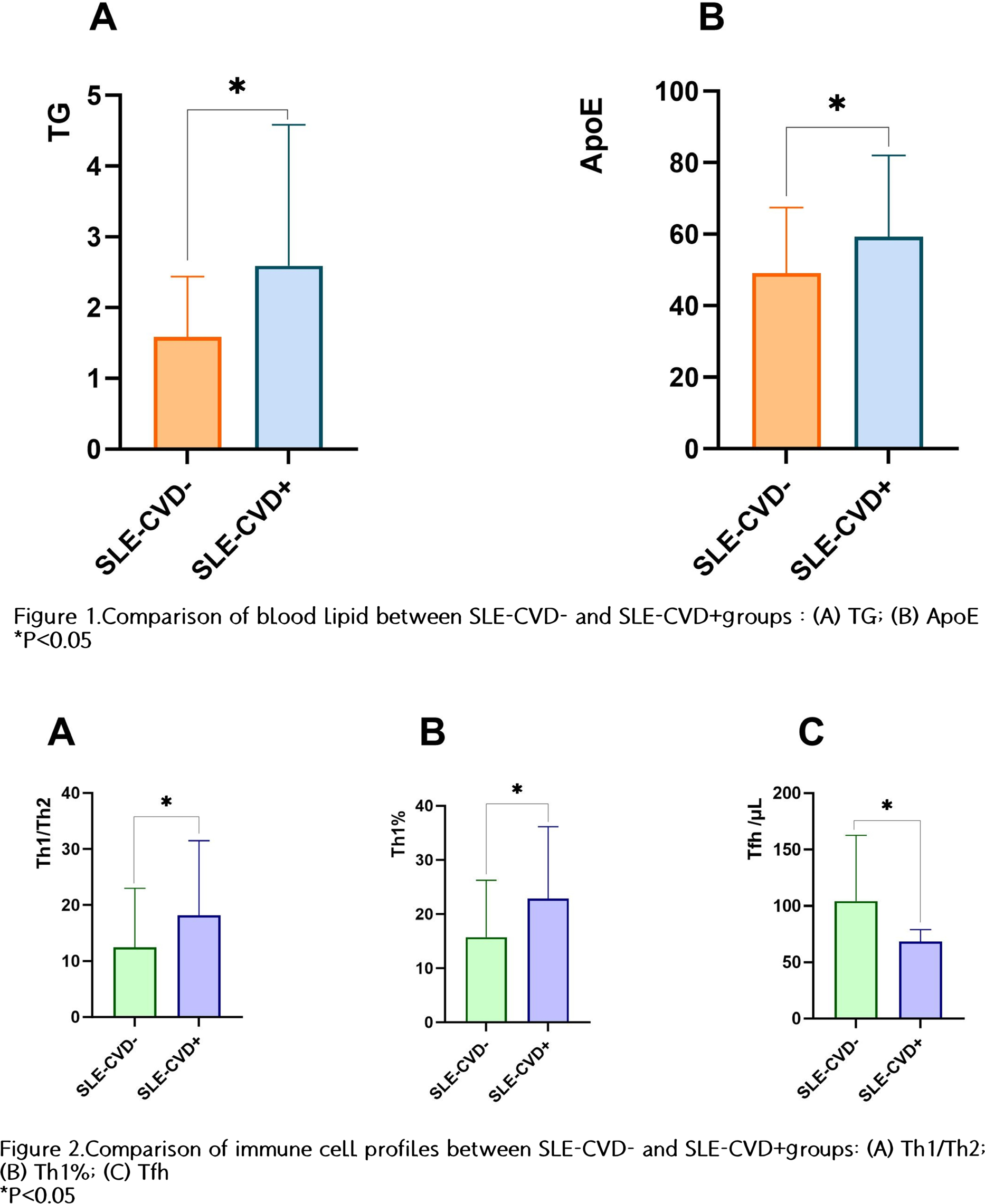
Results: Among these patients, 54 cases (4.08%) had CVD, while 1,271 cases (95.92%) did not exhibit CVD( Table 1 ). There was no significant difference in disease activity, as measured by the SLADAI score, between the SLE-CVD+ and SLE-CVD- groups. Additionally, smoking status and body mass index (BMI) did not show statistically significant differences between the groups. In contrast, significant differences were observed in clinical laboratory indicators between the two groups.In lipid-related indicators, the levels of TG (P=0.047) and Apo E (P=0.044) were significantly elevated in the SLE-CVD+ group compared to the SLE-CVD- group( Figure 1 ). Furthermore, in liver function indicators, the levels of fibronectin (Fn, P<0.001) and B factor (P=0.032) were significantly higher in the SLE-CVD+ group than in the SLE-CVD- group.In the context of renal function indicators, the levels of β2 microglobulin (P=0.045), α1 microglobulin (P=0.005), retinol binding protein (P=0.019), and urea nitrogen (P=0.022) were significantly elevated in the SLE-CVD+ group. In terms of immune cell profiles, compared with the SLE-CVD- group, the percentages of Th1 (P=0.011) and the Th1/Th2 ratio (P=0.042) in the SLE-CVD+ group were significantly increased, while the absolute number of Tfh (P=0.033) was significantly lower( Figure 2 ).
Conclusions: SLE patients with cardiovascular complications display a distinct immunometabolic phenotype characterized by Th1-skewed immunity, dyslipidemia, and evidence of hepatic and renal dysfunction. The elevated Th1/Th2 ratio suggests that pro-inflammatory Th1 responses may contribute to endothelial injury and atherogenesis in this population. These findings support the integration of immune profiling and metabolic monitoring into cardiovascular risk assessment for SLE patients.
Table 1. Comparison of demographic and cardiovascular risk factors in SLE-CVD+ and SLE-CVD- group
REFERENCES: [1] M.L. Hermansen, J. Lindhardsen, C. Torp-Pedersen, M. Faurschou, S. Jacobsen, The risk of cardiovascular morbidity and cardiovascular mortality in systemic lupus erythematosus and lupus nephritis: a Danish nationwide population-based cohort study, Rheumatology (Oxford, England) 56(5) (2017) 709-715.
[2] J. Frostegård, Systemic lupus erythematosus and cardiovascular disease, Journal of internal medicine 293(1) (2023) 48-62.
[3] M.A. Ameer, H. Chaudhry, J. Mushtaq, O.S. Khan, M. Babar, T. Hashim, S. Zeb, M.A. Tariq, S.R. Patlolla, J. Ali, S.N. Hashim, S. Hashim, An Overview of Systemic Lupus Erythematosus (SLE) Pathogenesis, Classification, and Management, Cureus 14(10) (2022) e30330.
Acknowledgments: NIL.
Disclosure of Interests: None declared.