fetching data ... 
Background: Systemic lupus erythematosus (SLE) predominantly affects young women, and lupus nephritis (LN) has a major impact on patient prognosis. In recent years, the incidence of late-onset SLE has been increasing, and the evaluation and management of LN in older patients are often challenging because of age-related declines in renal function and the presence of comorbidities. Although previous studies have suggested that late-onset LN is characterized predominantly by chronic pathological changes, its clinical features, detailed histopathological findings, and long-term outcomes have not yet been fully elucidated.
Objectives: To elucidate the clinical and renal histopathological characteristics of late-onset lupus nephritis.
Methods: Consecutive patients newly diagnosed with biopsy-proven active LN (class III, IV, or V) from 2008 to 2024 at our hospital were included. All patients received induction therapy with glucocorticoids (GCs) at doses ≥0.5 mg/kg. Patients were classified into two groups: a late-onset group, defined as those aged ≥50 years at LN diagnosis, and an early-onset group, defined as those aged <50 years. Clinical characteristics and renal histopathological findings were compared between the two groups. Complete renal response (CRR) was defined as urinary protein-to-creatinine ratio (UPCR) <0.5g/gCr and an estimated glomerular filtration rate (eGFR) that did not worsen by 10% or more from baseline or an eGFR ≥90 mL/min/1.73 m 2 . Deterioration of renal function was defined as a decline in eGFR of >30% from baseline.
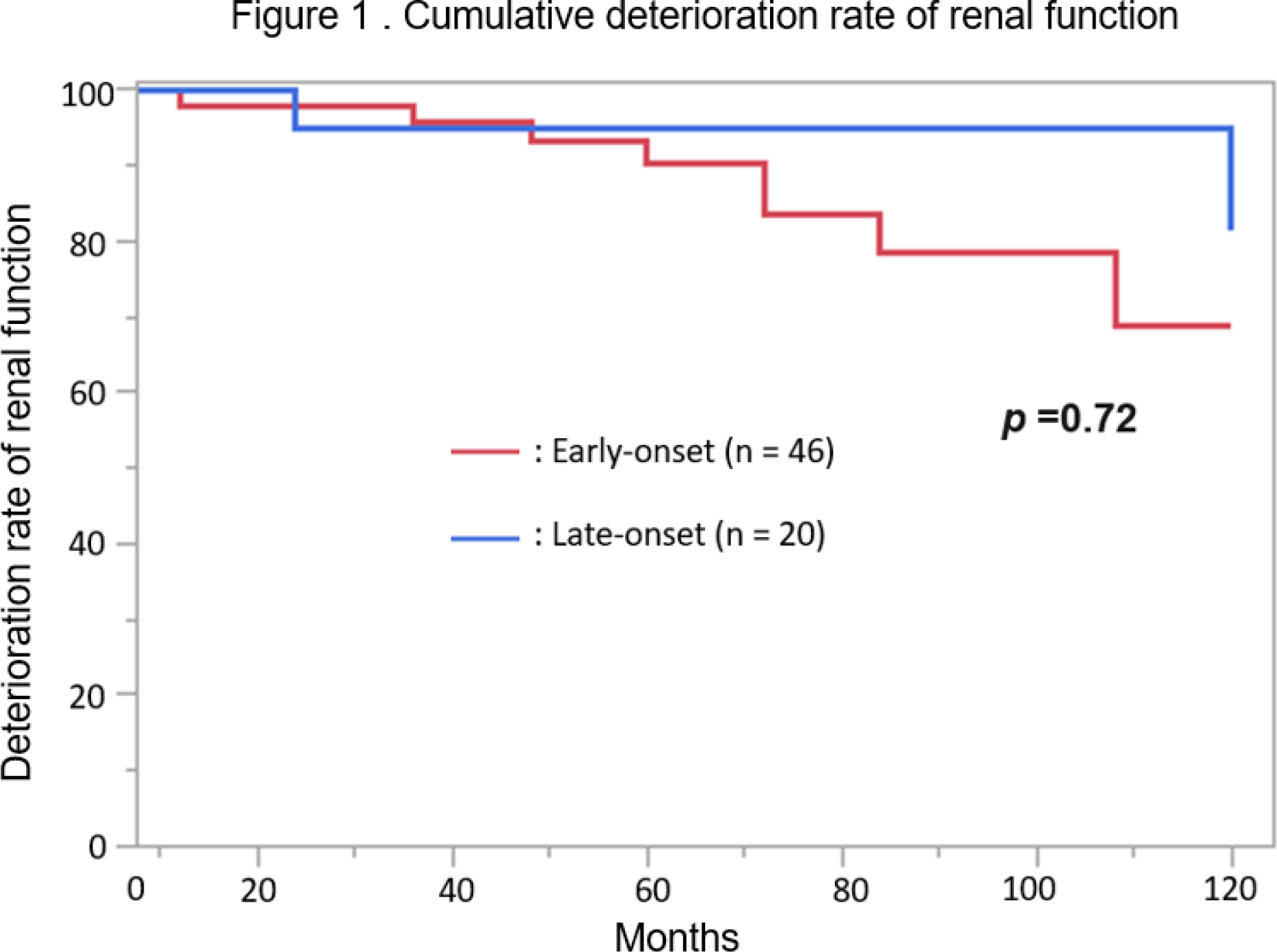
Results: A total of 81 patients with LN (class III/IV: 38; class III/IV + V: 18; class V: 25) were analyzed. Twenty-five patients (30.9%) were classified into the late-onset LN group. The mean age was 58 years in the late-onset group and 39 years in the early-onset group, and the proportion of female patients was comparable between the two groups (80.0% vs. 75.0%, p = 0.78). There were no significant differences in the prevalence of disease-specific autoantibodies, hypocomplementemia, or UPCR (1.9 vs. 1.8 g/gCr, p = 0.95) at treatment initiation. In terms of renal function, eGFR was significantly lower in the late-onset group (63.9 vs. 89.4 mL/min/1.73 m 2 , p < 0.01). Histologically, there were no significant differences in LN class distribution or activity index (3.9 vs. 3.0, p = 0.26) between the two groups, whereas the chronicity index was significantly higher in the late-onset group than in the early-onset group (3.1 vs. 1.8, p < 0.01). Detailed histopathological analyses revealed that the late-onset group had significantly higher scores for interstitial inflammation (0.6 vs. 0.2, p < 0.01), interstitial fibrosis (1.1 vs. 0.6, p < 0.01), tubular atrophy (1.0 vs. 0.6, p < 0.01), and glomerulosclerosis (1.0 vs. 0.6, p = 0.02). Induction therapy was administered similarly in both groups (initial GC dose: 46.8 vs. 48.2 mg/kg, p = 0.64; no significant differences in the types of immunosuppressive agents used). The CRR rate at 12 months after induction therapy was comparable between the two groups (76.5% vs. 75.0%, p = 1.00). Kaplan–Meier analysis demonstrated no significant difference in the long-term cumulative incidence of renal function decline between the two groups (p = 0.72, Figure 1).
Conclusions: Although late-onset LN is characterized by more prominent chronic renal histopathological lesions and reduced renal function at diagnosis, standard treatment enables CRR rates and long-term preservation of renal function comparable to those observed in early-onset LN.
REFERENCES: NIL.
Acknowledgments: NIL.
Disclosure of Interests: None declared.