fetching data ... 
Background: Systemic lupus erythematosus (SLE) is an autoimmune disease involving multi-organ inflammation and dysregulated adaptive immunity [1]. Current standard therapies, including glucocorticoids, conventional immunosuppressants, and biologics, are often limited by incomplete efficacy, significant toxicities, or high cost. Sirolimus, an inhibitor of the mechanistic target of rapamycin complex 1 (mTORC1)[2], has shown promise in preclinical models of SLE by promoting regulatory T (Treg) cell function and restraining pro-inflammatory T helper 17 (Th17) cell responses [3]. However, comprehensive clinical data on its efficacy and immunomodulatory profile in patients with SLE remain scarce.
Objectives: This study aimed to evaluate the clinical efficacy of sirolimus in the treatment of SLE and its effects on immune cells and related biomarkers.
Methods: A total of 142 SLE patients who met the 2019 ACR/EULAR classification criteria for SLE were retrospectively included from the Second Hospital of Shanxi Medical University between 2015 and 2024. Based on their treatment regimens, the patients were divided into a Sirolimus group, a Conventional Therapy group, and a Biologics group. Clinical data and medication details were obtained from electronic medical records. Collected indicators included the disease activity index (SLEDAI), peripheral blood Treg and Th17 cell counts, as well as markers such as C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR). Statistical analysis was performed using SPSS and GraphPad Prism. For normally distributed data, paired t-tests and independent samples t-tests were applied; for non-normally distributed data, the Wilcoxon signed-rank test and the Mann–Whitney U test were used. Comparisons between categorical variables were conducted using the chi-square test. A P -value < 0.05 was considered statistically significant.
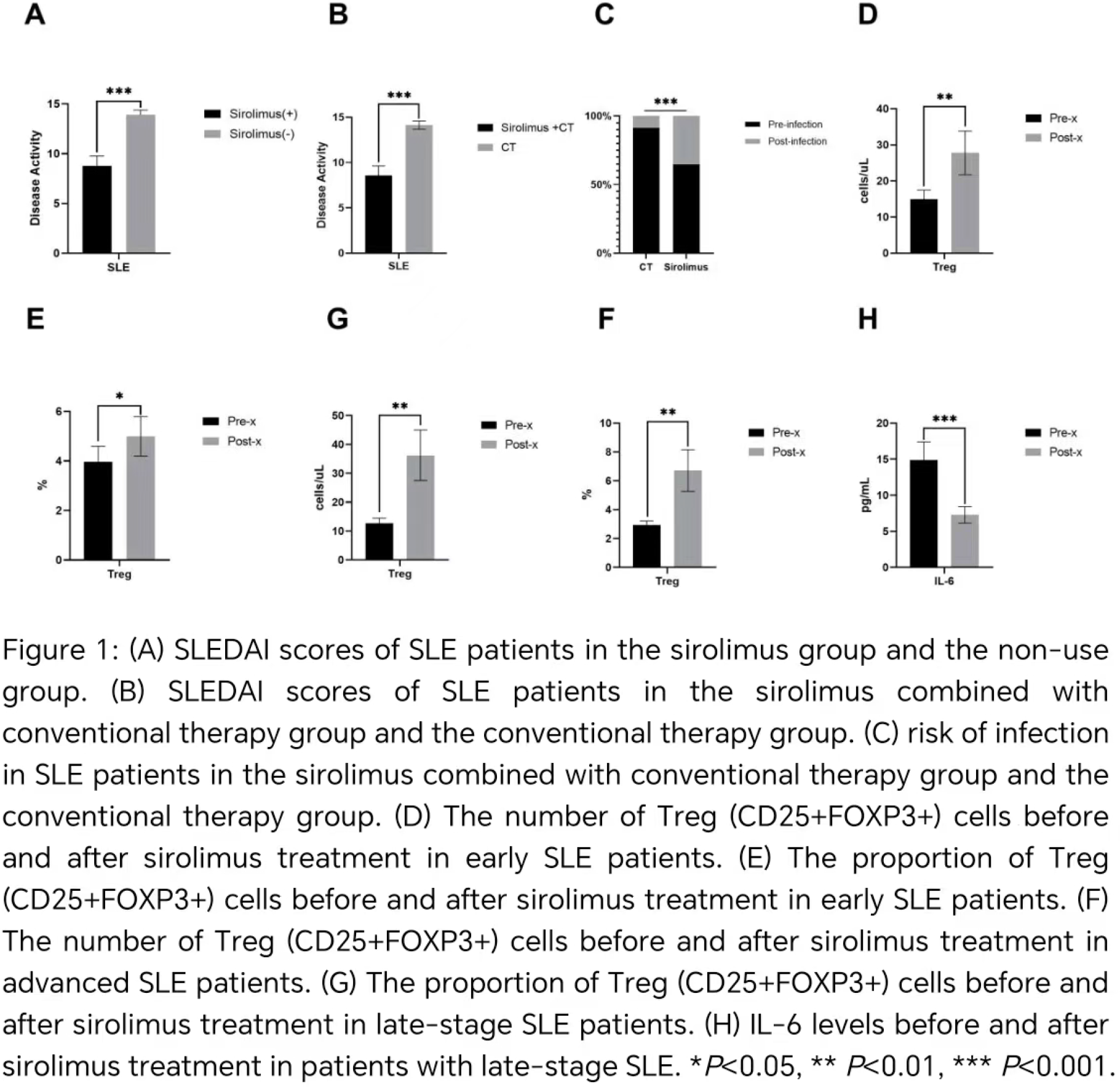
Results: The SLEDAI score was significantly lower in the sirolimus group compared to the non-sirolimus group (p < 0.001). Similarly, the combined sirolimus and conventional therapy group exhibited a lower score than the conventional therapy-alone group (p < 0.001), though it was associated with a higher risk of infection (χ 2 (1, N=136) = 14.953, p < 0.001). No significant differences were observed in disease activity or infection risk between the combined sirolimus and conventional therapy group and the combined biologics and conventional therapy group. Furthermore, sirolimus use showed no association with the risk of lupus nephritis.
Compared to the non-sirolimus group, the sirolimus group demonstrated increased Treg cell count and proportion (p = 0.001; p = 0.01) and decreased Th17 cell count and proportion (p = 0.0356; p = 0.048). Longitudinal analysis within the same patients before and after sirolimus treatment revealed an increase in Treg cell count and proportion (both p < 0.001), elevated complement C3 and C4 levels (both p = 0.002), and reduced creatinine and IL-6 levels (both p < 0.001). Following sirolimus treatment, patients showed elevated Treg cell counts and proportions (all p < 0.05). Early-stage patients exhibited declines in CRP and ESR (p < 0.05), while late-stage patients demonstrated a reduction in IL-6 (p<0.001).
Conclusions: Sirolimus effectively reduces disease activity in SLE and promotes a favorable shift in immune balance by expanding Tregs and suppressing Th17 cells. Its clinical efficacy is comparable to biologic therapies, with additional benefits on complement restoration and renal biomarker improvement. Although associated with a measurable infection risk, its overall immunomodulatory profile and potential cost-effectiveness support its consideration as a valuable therapeutic alternative for SLE, particularly in patients with refractory disease or specific immunological phenotypes.
REFERENCES: [1] M. Kiriakidou, C.L. Ching, Systemic Lupus Erythematosus, Annals of internal medicine 172(11) (2020) Itc81-itc96.
[2] K. Gollomp, D.T. Teachey, TORing the impact of sirolimus on immune health, Blood 141(3) (2023) 212-214.
[3] D. Cluxton, A. Petrasca, B. Moran, J.M. Fletcher, Differential Regulation of Human Treg and Th17 Cells by Fatty Acid Synthesis and Glycolysis, Frontiers in immunology 10 (2019) 115.
Acknowledgments: NIL.
Disclosure of Interests: None declared.