fetching data ... 
Background: Systemic lupus erythematosus (SLE) is a chronic systemic autoimmune disease that predominantly affects women of reproductive age. Late-onset SLE, defined as disease onset after the age of 50 years, accounts for approximately 2-20% of SLE cases. However, how the rate of organ damage accumulation varies according to age at disease onset remains insufficiently characterized.
Objectives: To compare the clinical and serological characteristics of juvenile-, adult-, and late-onset SLE patients and to evaluate differences in cumulative organ damage and the rate of damage accumulation across these groups.
Methods: A total of 528 patients with systemic lupus erythematosus followed at the Rheumatology Clinic of Gazi University between 2000 and 2025 were included. Cumulative organ damage was assessed using the Systemic Lupus International Collaborating Clinics/American College of Rheumatology Damage Index (SLICC/ACR Damage Index (SDI).The annualized SDI progression rate was calculated as the total increase in SDI score divided by disease duration (years) and compared across juvenile, adult, and late-onset subgroups. Differences in SDI domains and their association with annualized damage progression were evaluated across onset groups. A Poisson regression model was fitted with disease duration included as an offset variable, and overdispersion was adjusted using the Pearson scaling parameter. Age at diagnosis was included as the main independent variable. This approach allowed partial separation of the effects of disease duration from age-related factors. Sensitivity analyses were performed in patients with documented organ damage (SDI ≥1), in which annualized SDI progression rates, total SDI scores, and the distribution of SDI presence were compared between groups.
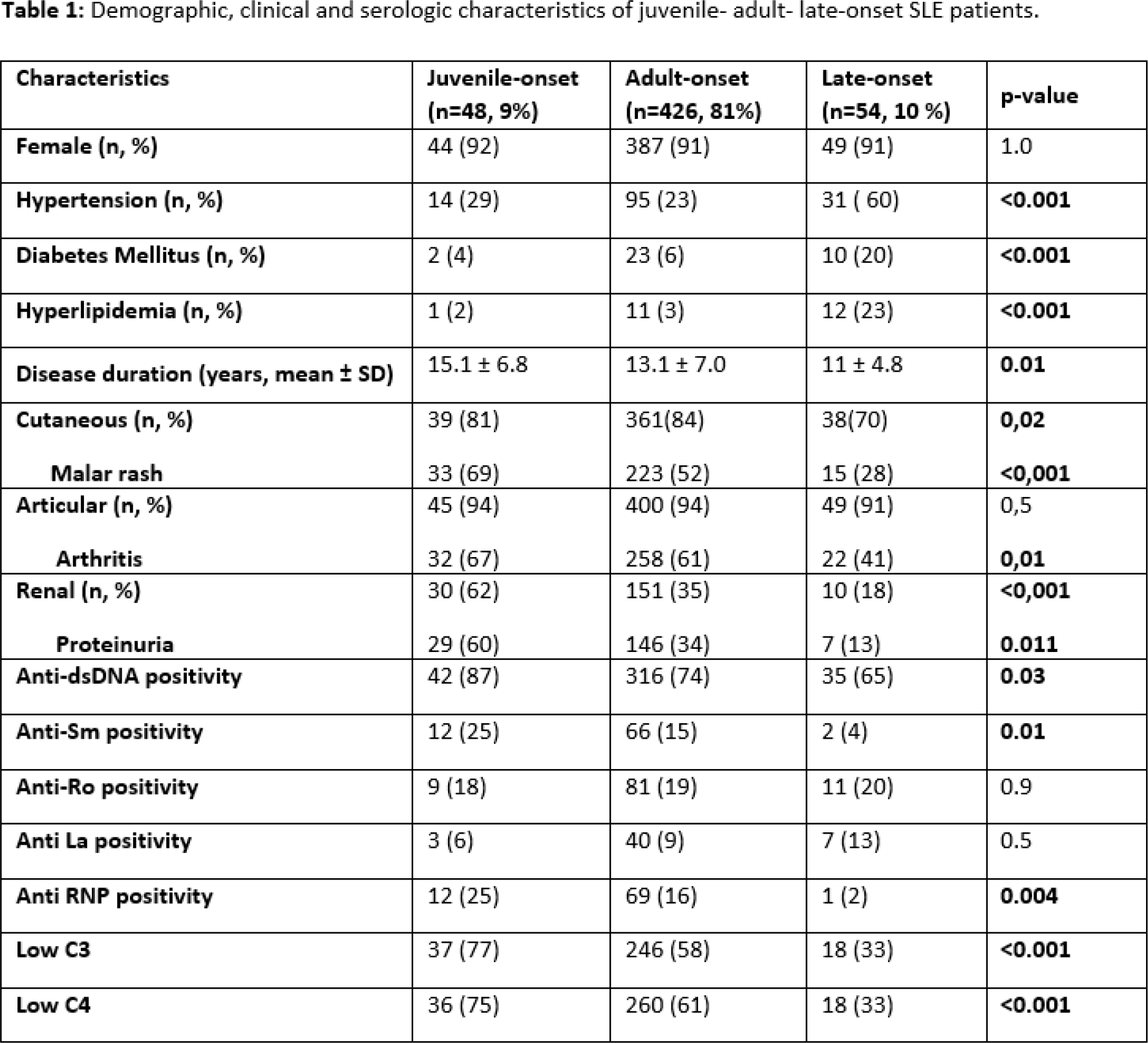
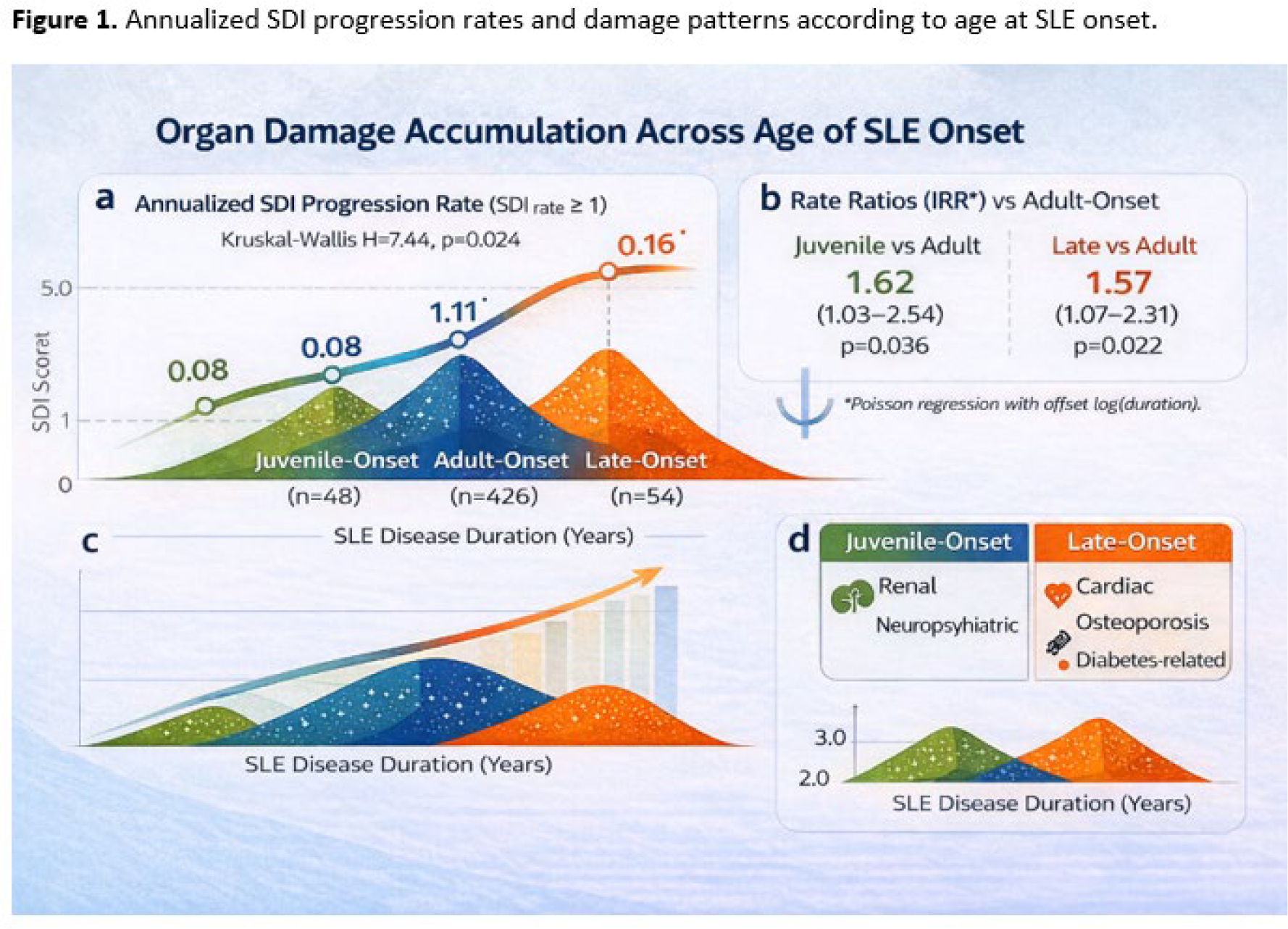
Results: The 528 patients were divided into three groups according to age, with more women in all age groups. Patients in the juvenile age group had the longest follow-up period. Considering clinical findings, cutaneous and renal involvement, as well as arthritis, were more frequently observed in juvenile- and adult-onset groups (Table 1). Annualized SDI progression rates differed significantly according to age at disease onset. The lowest rate was observed in juvenile-onset SLE, while the highest rate was seen in late-onset disease (Figure 1a). Despite longer disease duration, juvenile-onset patients exhibited lower cumulative damage and slower crude damage accrual compared with late-onset patients. In the Poisson regression model adjusted for disease duration with an offset, no significant difference was found in the annualized SDI progression rates between the juvenile and late-onset SLE groups; however, both groups were found to have a significantly higher annualized SDI progression rate compared to adult-onset SLE (Figure 1b). Analysis of SDI domains revealed distinct damage phenotypes. Juvenile-onset SLE was characterized by higher frequencies of renal and neurological damage, whereas late-onset SLE showed a predominance of cardiac, musculoskeletal, and metabolic (diabetes-related) damage (Figure 1c). Importantly, cardiac, renal, neurological, and diabetes-related damage items were the strongest drivers of accelerated annualized SDI progression, indicating a disproportionate contribution of these domains to rapid damage accumulation.
Conclusions: In addition to the presence of organ damage, the rate of damage accumulation should be considered an essential outcome in the long-term follow-up of patients with SLE, particularly when comparing disease phenotypes across different age-at-onset groups. Despite longer disease duration in the juvenile-onset group, the relatively low annualized SDI progression rates indicate that damage accumulation is not solely driven by disease duration but is also influenced by distinct patterns of involvement across SDI subdomains.
Table 1 . Demographic, clinical and serologic characteristics of juvenile- adult- late-onset SLE patients.
Annualized SDI progression rates and damage patterns according to age at SLE onset.
REFERENCES: NIL.
Acknowledgments: NIL.
Disclosure of Interests: None declared.