fetching data ... 
Background: Systemic Lupus Erythematosus (SLE) is a chronic systemic autoimmune disease with clinical manifestations ranging from fatigue and joint pain to severe organ damage, which can significantly impact Health-Related Quality of Life (HR-QoL). The European Alliance of Associations for Rheumatology (EULAR) recommendations for the management of SLE state that non-pharmacological interventions, including regular exercise, are important to improve long-term outcomes. The World Health Organization (WHO) provides evidence-based recommendations on the amount of physical activity required to offer significant health benefits and reduce health risk, which also apply to patients with Rheumatic and Musculoskeletal Diseases.
The modified Short QUestionnaire to ASsess Health-enhancing physical activity (mSQUASH) is a questionnaire that measures physical activity in different domains, including commute, work or school, household, and leisure activities, sports and exercise [1]. The feasibility, validity and reliability of the mSQUASH for measuring daily physical activity have already been shown in patients with axial spondyloarthritis and Sjögren’s disease [1,2]. It is expected that the mSQUASH can also be used to measure physical activity in patients with SLE.
Objectives: To conduct field testing and clinical validation of the mSQUASH, and to provide insight into types and amounts of physical activity performed by patients with SLE, their adherence to the WHO recommendations and the association of physical activity with HR-QoL.
Methods: Patients with clinical diagnosis of SLE were included. Field testing consisted of semi-structured face-to-face interviews (n=10). Construct validity (n=95) was assessed using Spearman correlations between the mSQUASH and other Patient-Reported Outcome Measures (PROMs) of disease activity (patient GDA), fatigue (MFI), health status (EQ-5D-5L), HR-QoL (SF-36) and limitations in daily activity (HAQ-DI). We hypothesized that there would be fair to moderate associations between the mSQUASH and other PROMs, as they assess related but reflect different constructs. Test-retest reliability (n=78) was assessed using Intraclass Correlation Coefficients (ICCs) and Bland-Altman analysis. Insight into types and amounts of physical activity, and adherence to WHO recommendations (aerobic physical activity: ≥150 minutes moderate-intensity physical activity, ≥75 minutes vigorous-intensity physical activity or a combination of both, and muscle-strengthening activities: involving all major muscle groups, ≥2 days per week) was based on the mSQUASH. Associations of physical activity (mSQUASH minutes per week) with HR-QoL (SF-36) were assessed using univariable linear regression analyses and multivariable linear regression analyses to correct for potential confounders (age, sex, Body Mass Index (BMI), Systemic Lupus Erythematosus Disease Activity Index (SLEDAI) and systemic medication use).
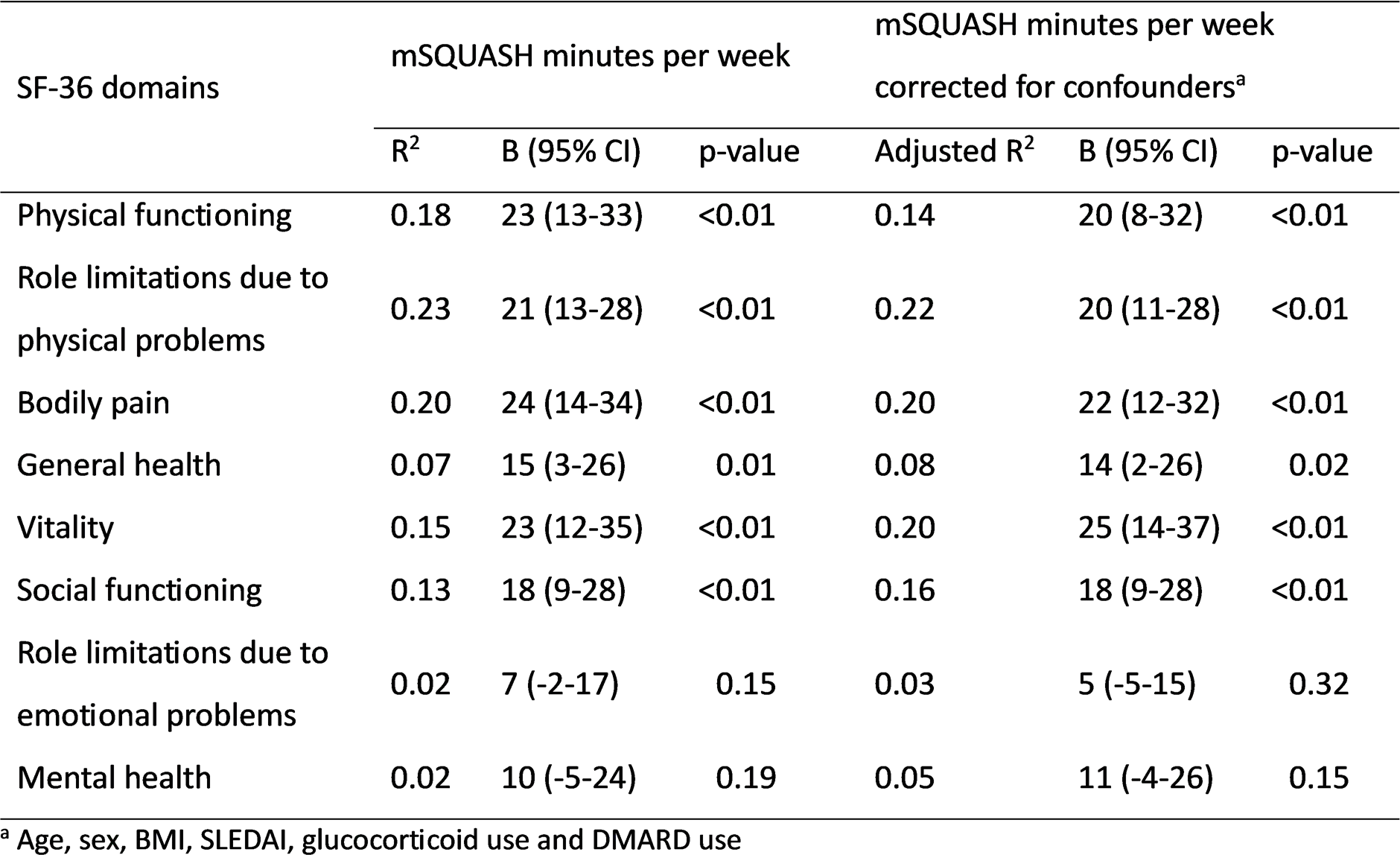
Results: Included SLE patients were 45±15 years old, 85% were female, 81% used hydroxychloroquine, 38% used other Disease-Modifying Anti-Rheumatic Drugs (DMARDs), 10% used glucocorticoids and they had a median SLEDAI score of 0 (0-2). All patients perceived the mSQUASH as relevant and linguistically clear. Mean time to complete the mSQUASH was 4.1±0.9 minutes. Fair to moderate associations between the mSQUASH total activity score and other PROMs were found (e.g. MFI physical fatigue: ρ=-0.35, EQ-5D-5L total score: ρ=-0.38, EQ-5D-5L mobility: ρ=-0.43, SF-36 physical functioning ρ=0.38 and HAQ-DI common daily activities: ρ=-0.31). The work domain showed strongest associations with other PROMs (e.g. patient GDA: ρ=-0.34, MFI physical fatigue: ρ=-0.39, EQ-5D-5L usual activity: ρ=-0.48, SF-36 physical functioning: ρ=0.61, HAQ-DI total score: ρ=-0.47 and HAQ-DI common daily activities: ρ=-0.47). Test-retest reliability of the mSQUASH was good (ICC=0.72). Bland-Altman analysis showed a small mean difference (585) between the two assessments, not significantly different from zero, indicating that there is no systematic bias. The 95% limits of agreements were wide (-4633, 5802). Regular household activities (98%), walking (93%), intensive household activities (85%) and regular work (69%) were most frequently performed by patients with SLE. Two-thirds of the patients participated in sports and exercises, with health club exercises (i.e. fitness and group lessons) being the most common (Figure 1). In total, 33% of the patients with SLE adhered to the WHO recommendations. Almost all patients (95%) fulfilled the aerobic physical activity component and 33% of the patients fulfilled the muscle-strengthening component. Univariable linear regression showed significant associations between the mSQUASH and SF-36 domains physical functioning, role limitations due to physical problems, bodily pain, general health, vitality and social functioning (Table 1). All remained statistically significant after correcting for potential confounders, with strongest association for role limitations due to physical problems, bodily pain and vitality.
Conclusions: The mSQUASH is a feasible, valid and reliable questionnaire to measure daily physical activity in different domains in patients with SLE. Almost all patients performed aerobic physical activity, but muscle-strengthening activities should be performed more often. Spending more time on physical activity was significantly associated with better HR-QoL.
A) Types of physical activity performed by patients with SLE (n=95) and B) minutes per week in the subgroup of patients performing these activities
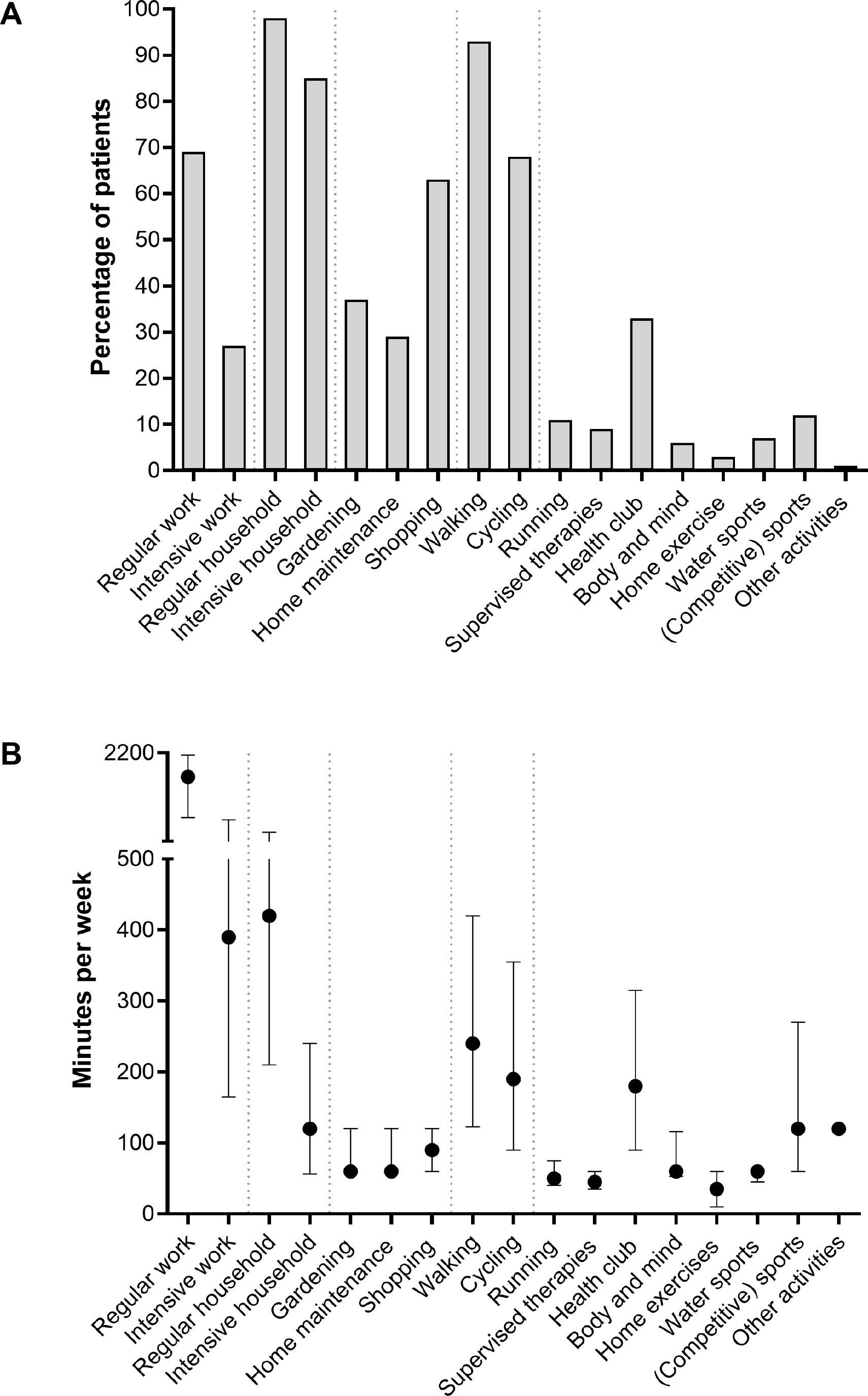
Table 1. Associations of physical activity with HR-QoL in patients with SLE (n=95)
REFERENCES: [1] van der Kraan et al. RMD Open. 2024;10.
[2] Ausma et al. Clin Exp Rheumatol. 2024;2468-2473.
Acknowledgments: NIL.
Disclosure of Interests: Daphne Harmsen: None declared, Helene Kokol: None declared, Davy Paap: None declared, J.P.L Spoorenberg: None declared, Karina de Leeuw: None declared, Suzanne Arends Consultant for Argenx, BMS, Novartis