fetching data ... 
Background: Despite major advances in the biological understanding of systemic lupus erythematosus (SLE), many late-phase SLE clinical trials have failed to meet primary efficacy endpoints. A widely recognised contributor is the performance of disease-activity outcome measures, which remain vulnerable to assessor variability, inconsistent application, and limited operational feasibility at scale. The BILAG-2004 index underpins key composite endpoints, including the SLE Responder Index (SRI-4), and is regarded as conceptually superior to SLEDAI due to its organ-based structure, sensitivity to partial change, and alignment with physician intent to treat. However, these strengths are undermined by substantial practical barriers. BILAG-2004 is complex and rule-driven, requiring extensive training and sustained use to maintain fluency. In global multicentre trials and busy outpatient clinics, this results in inconsistent scoring, protocol deviations, data queries, and reliance on central adjudication, increasing monitoring costs and reducing confidence in trial outcomes among sponsors and regulators.
Objectives: To develop and evaluate EasyBILAG-Digital , a cross-platform digital implementation of BILAG-2004 designed to remove long-standing operational barriers to accurate BILAG scoring. We aimed to evaluate whether EasyBILAG-Digital could enhance the practical delivery of BILAG-2004 in routine care and clinical trials by improving user experience, reducing fluency-related variability, and enabling auditable, standardised, and secure digital capture of BILAG data.
Methods: EasyBILAG-Digital is available via a secure web application and native Android and iOS platforms. The system fully encodes the BILAG-2004 glossary, attribution rules, and scoring logic, guiding assessors through each organ domain while automatically calculating final grades. Common BILAG scoring errors and activity misattributions are subject to additional light-touch validation prompts, designed to prevent frequent rule violations while preserving assessor autonomy. Real-time validation prevents missing data, inconsistent responses, and rule violations, producing fully auditable outputs suitable for electronic health records and trial databases. Specialist lupus clinicians independently scored identical simulated SLE cases using paper BILAG-2004 and EasyBILAG-Digital. Cases were stratified by complexity to reflect routine follow-up and complex trial assessments. Outcomes included time to completion, scoring accuracy (item, domain, and case level), and user experience. Paired Wilcoxon signed-rank tests (and paired t-tests where appropriate) assessed timing, chi-square tests compared accuracy distributions, and two-proportion z-tests evaluated completely correct case rates. User experience was assessed using a 10-item Likert questionnaire (0–5).
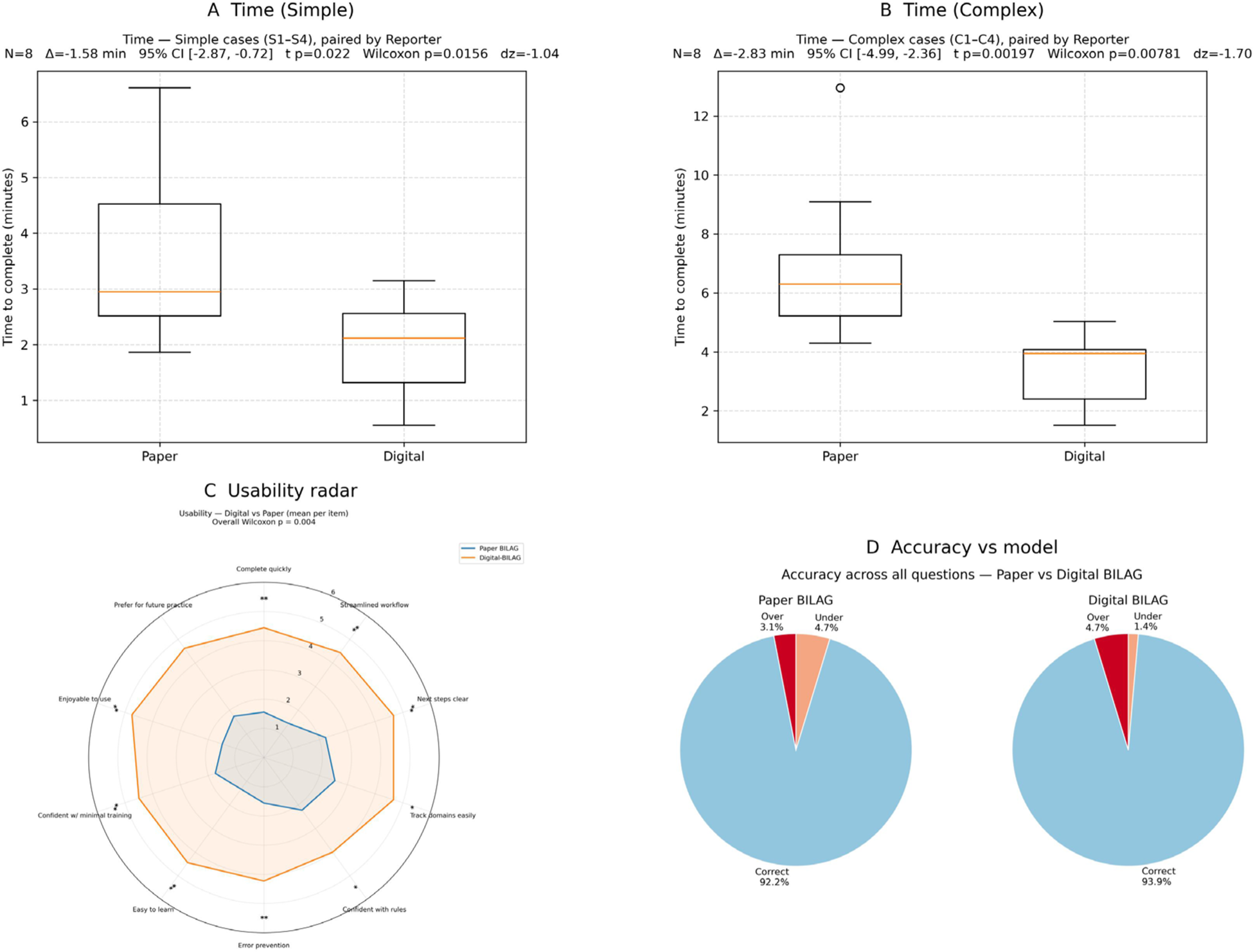
Results: EasyBILAG-Digital was associated with faster case completion. Median completion time was reduced by 1.6 minutes for simple cases (p=0.016) and 2.8 minutes for complex cases (p=0.002), without reduction in scoring accuracy. Domain-level scoring accuracy was comparable between EasyBILAG-Digital and paper BILAG-2004 (92.2 percent versus 93.9 percent). User experience scores were higher with EasyBILAG-Digital, with mean usability scores increasing from 1.8 to 4.5 (p=0.004). Significant improvements were observed across workflow efficiency, clarity of scoring, confidence in rule application, error prevention, training burden, and overall usability. EasyBILAG-Digital generated structured outputs compatible with REDCap, CSV, XLS, and SQLite databases via Cloudflare, with summary outputs exportable to electronic health records. Native iOS builds were deployed via Apple TestFlight, with beta test access available on application.
Conclusions: EasyBILAG-Digital represents a practice-changing advance in SLE disease-activity assessment. By addressing the operational, rather than conceptual, limitations of BILAG-2004, it enables reliable organ-based scoring at scale. For clinical trials, standardised and auditable data capture reduces inter-site variability, data queries, and reliance on central adjudication. These are major drivers of monitoring cost and endpoint uncertainty, and their reduction strengthens confidence in BILAG-based endpoints for regulatory review by agencies such as the FDA and EMA. In routine care, the use of BILAG supports comprehensive, organ-based assessment of lupus activity, and cross-platform availability enables real-time use in busy clinics without increasing clinician workload. EasyBILAG-Digital therefore provides a scalable, regulator-ready solution that bridges high-quality clinical assessment with modern trial methodology.
Take-home message
EasyBILAG-Digital removes the practical barriers that have limited BILAG-2004 for two decades, transforming it into a scalable, regulator-ready endpoint for SLE trials and routine care.
REFERENCES: [1] Furie R, Morand EF, Bruce IN, et al. Type I interferon inhibitor anifrolumab in active systemic lupus erythematosus. N Engl J Med. 2019;381:211–221.
[2] Isenberg DA, Rahman A, Allen E, et al. BILAG 2004 development and validation. Rheumatology (Oxford). 2005;44:902–906.
[3] Yee CS, Farewell V, Isenberg DA, et al. Revised British Isles Lupus Assessment Group 2004 index. Rheumatology (Oxford). 2005;44:902–906.
[4] Carter L, et al. Easy-BILAG: improving the accuracy and efficiency of BILAG-2004 scoring. Rheumatology (Oxford). 2021;60:2087–2096.
Acknowledgments: NIL.
Disclosure of Interests: Jack Arnold Alumis, UCB, Novartis, Roche,, Bhavika Sethi: None declared, Lucy Marie Carter Alumis, Novartis, UCB, Edward M. Vital F. Hoffmann-La Roche Ltd/Genentech, Inc., AstraZeneca, Otsuka, Novartis, Eli Lilly and Company, Pfizer, Merck, AbbVie and UCB., AstraZeneca, UCB, Novartis.