fetching data ... 
Background: Raynaud Phenomenon (RP) may cause digital ulcers, auto-amputation, and reduced quality of life. Current treatments are often poorly tolerated or contraindicated in scleroderma. Nicotinamide (vitamin B3) is an indirect vasodilator with anti-inflammatory and DNA repair effects. Low B3 levels (skin/organs) have been linked to scleroderma-related fibrosis via NADase (CD38) upregulation [1]. Compared with standard RP therapies, B3 is inexpensive, doses of 500 mg twice daily orally are well tolerated and safe [2]. B3’s effect in scleroderma RP has not been studied.
Objectives: To evaluate whether B3 supplementation is a safe and effective adjunctive treatment for primary and scleroderma RP. Primary endpoints: B3 adherence and side-effects
Changes in nailfold videocapillaroscopy (NVC) patterns/parameters Changes in validated patient-related outcome measures (PROMs):
RP frequency/severity (Raynaud Condition Score [RCS] diary)
RP-related quality of life (Short-Form Assessment of Systemic Sclerosis-Associated Raynaud’s Phenomenon’ [SF-ASRAP] questionnaire)
Methods: Inclusion Criteria
Age 18–80 years
Diagnosis of RP as defined by the ‘International consensus criteria for the diagnosis of RP’ [3]
For secondary RP, must have scleroderma
No planned vasoactive medication changes during the study
No planned travel outside the study region during the study (to account for any variations in weather)
Exclusion Criteria
Secondary RP from non-scleroderma causes
Inability to undergo NVC (eg.nail polish; caffeine on the day)
Current nicotinamide/niacin use or contraindication
Pregnancy, breastfeeding, or intention to conceive within 3 months of the study
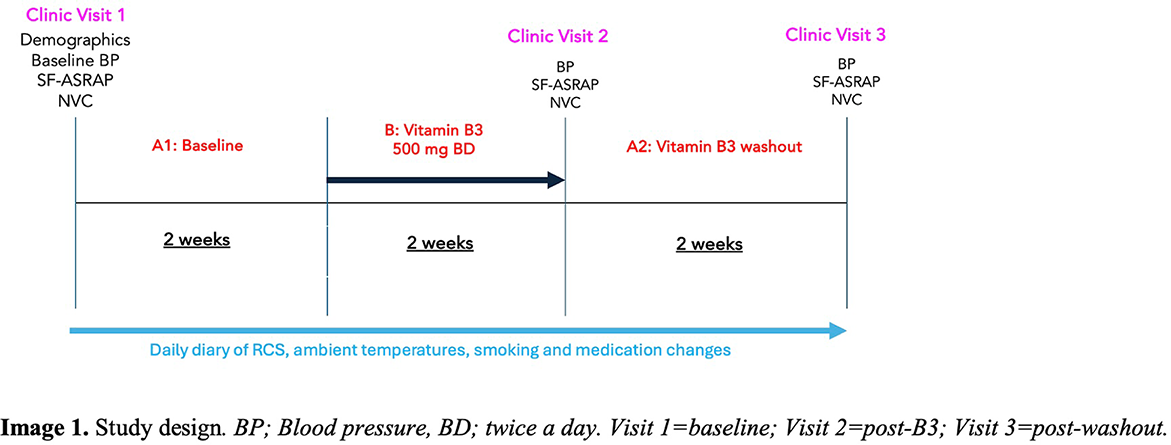
A 6-week prospective intervention study, 2 week per phase: A1 (baseline), B (B3 500mg twice a day orally), A2 (B3 washout) (figure 1).
Participants recruited from Canberra (Australia) and studied during winter. Rationale for 14 days of B3 was due to its short half-life, and use of similar study timeframes with other RP interventions (4). The NVC incorporated AI based on the validated CAPI-DETECT algorithm. Participants completed daily diaries recording RP frequency, duration, and severity; ambient temperature, and medication changes. During the B3 phase, diaries were kept for side effects and doses missed. Statistical analysis: RP stratified by type. NVC analysed by Student’s t-test and Pearson’s c 2 . SF-ASRAP and RCS assessed using MICD (Minimally Important Clinical Difference) and PASS (Patient Acceptable Symptom State) cut-offs, adjusted for age and ambient temperature.
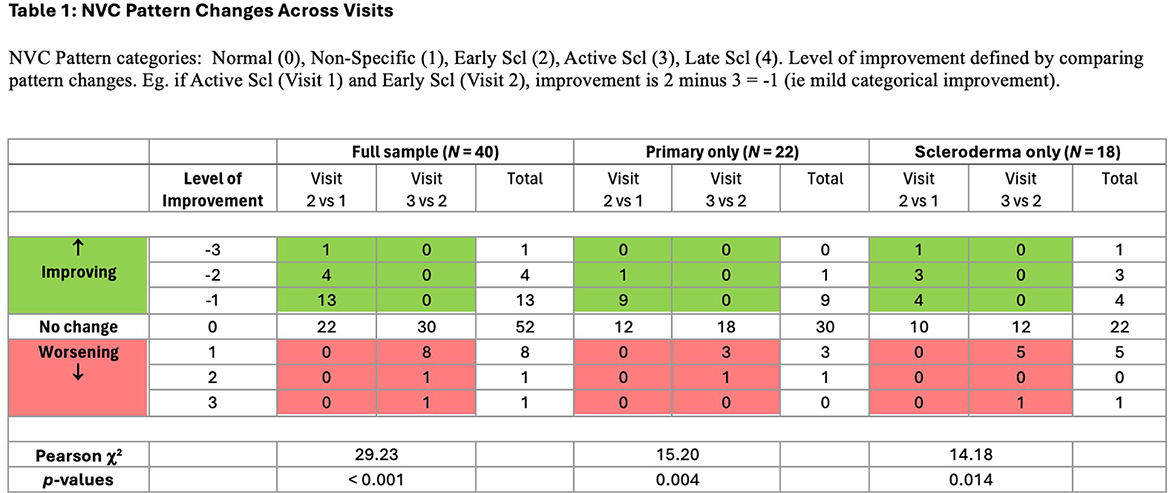
Results: 40 participants enrolled: 22 primary RP;18 scleroderma RP. Scleroderma participants were older (57.4 vs 45.1 years, p=0.01); other demographics and baseline RP management similar. Mean RP onset 33 years; 80% female; 88.5% Caucasian. No significant medication changes during the study. High adherence: 99.5% (N=1672/1680) diary entries completed; 1.3% (N=14/1120) B3 doses missed. Adverse events minor (12.5%; N=5/40). No significant systolic BP changes observed. NVC patterns Significantly improved in 45% (N=18/40) of participants post-B3 (visit 2 vs 1) (10 primary, p=0.004; 8 scleroderma, p=0.014) (Table 1); benefits persisting visit 3 vs 1 in both groups (Table 1). NVC parameters Total cohort post-B3: increased mean percentage of normal capillaries, reduced abnormal shapes and giant capillaries (p<0.05). Decreased mean tortuosities comparing post-washout to post-B3 (p<0.05). SF-ASRAP Primary group: percentage meeting PASS was 45.5% at baseline, 77.3% post-B3, 72.7% post-washout. However, only the mean SF-ASRAP score at post-washout was significantly less than the PASS (p=0.02). MICD: only the comparison post-washout vs baseline was significant (p=0.03). Scleroderma group: percentage meeting PASS was 27.78% at baseline, 33.3% post-B3, 27.8% post-washout, but mean SF-ASRAP scores and MICD were not statistically significantly across phases. RCS Primary group: percentage meeting PASS was 65% at baseline, 85% post-B3, 80% post-washout. The mean scores post-B3 and post-washout significantly achieved PASS (p<0.01). MICD not met across phases. Scleroderma group: percentage meeting PASS was 44.4% at baseline, 50% post-B3, 55.5% post-washout. However, the mean score of those meeting the PASS at each phase was not significant. MICD not met.
Conclusions: Nicotinamide 500 mg BD for 14 days was safe in primary and scleroderma RP. Subjective improvement in RP severity and RP-related quality of life was found in primary RP (robust for age and ambient temperature) but not scleroderma RP. However, NVC showed significant objective improvements in both groups. Scleroderma microvasculature may be more resistant to vasodilation. Ongoing improvement during the washout phase could suggest B3 may induce functional microvascular effects beyond its pharmacological half-life. Larger RCTs with longer and/or higher dosing (especially for scleroderma) are warranted.
REFERENCES: [1] Sji B, Wenxia W, Korman B et al. 2021. Targeting CD38-dependent NAD+ metabolism to mitigate multiple organ fibrosis;
iScience
;
[2] Chen A, Martin A, Choy B et al. 2015. A phase 3 randomised trial of nicotinamide for skin-cancer chemoprevention. NEJM ; 373:1618-26.
[3] Maverakis E, Patel F, Kronenberg D et. al. 2014. International Consensus Criteria for the diagnosis of Raynaud’s Phenomenon’. J Autoimmun ; Feb-Mar:48-49:60-5.doi: 10.1016/j.jaut.2014.01.020.
[4] Shenoy P, Kumar S, Jha L et. al. 2010. Efficacy of tadalafil in secondary Raynaud’s phenomenon resistant to vasodilator therapy: a double-blind randomized cross-over trial; Rheum Oxford Academic ; 9;12.
Acknowledgments: NIL.
Disclosure of Interests: None declared.