fetching data ... 
Background: Pulmonary arterial hypertension (PAH) is one of the most challenging complications of systemic sclerosis (SSc) patients (pts). Selexipag, an oral selective prostacyclin IP-receptor agonist, has been shown to reduce the risk of PAH-related mortality/morbidity in a phase 3 trial 1 , including PAH-SSc pts 2 . Moreover, a recent real-life study has highlighted potential use of selexipag in refractory digiital ulcers (DU) in SSc 3 .
Objectives: This study aims to investigate the real-world persistency and long-term clinical outcomes of selexipag-treated SSc-PAH pts in the EUSTAR cohort and its effectiveness on SSc-DU.
Methods: Adult SSc pts recorded in the EUSTAR database up to October 2025, fulfilling the 2013 ACR/EULAR criteria, on treatment with selexipag. Pts who started selexipag within 6 months of first informative visit were incident users, and those on selexipag for >6 months were prevalent users. Risk assessment was calculated according to the COMPERA 2.0 four-strata model. Selexipag persistency was evaluated with Kaplan–Meier survival analysis. DU effectiveness was assessed by DUCAS scoring system. Follow-up data at 12 ± 3 months in incident pts were assessed including 6-minute walking test (6MWT), NYHA functional class, risk assessment and change in number in DU.
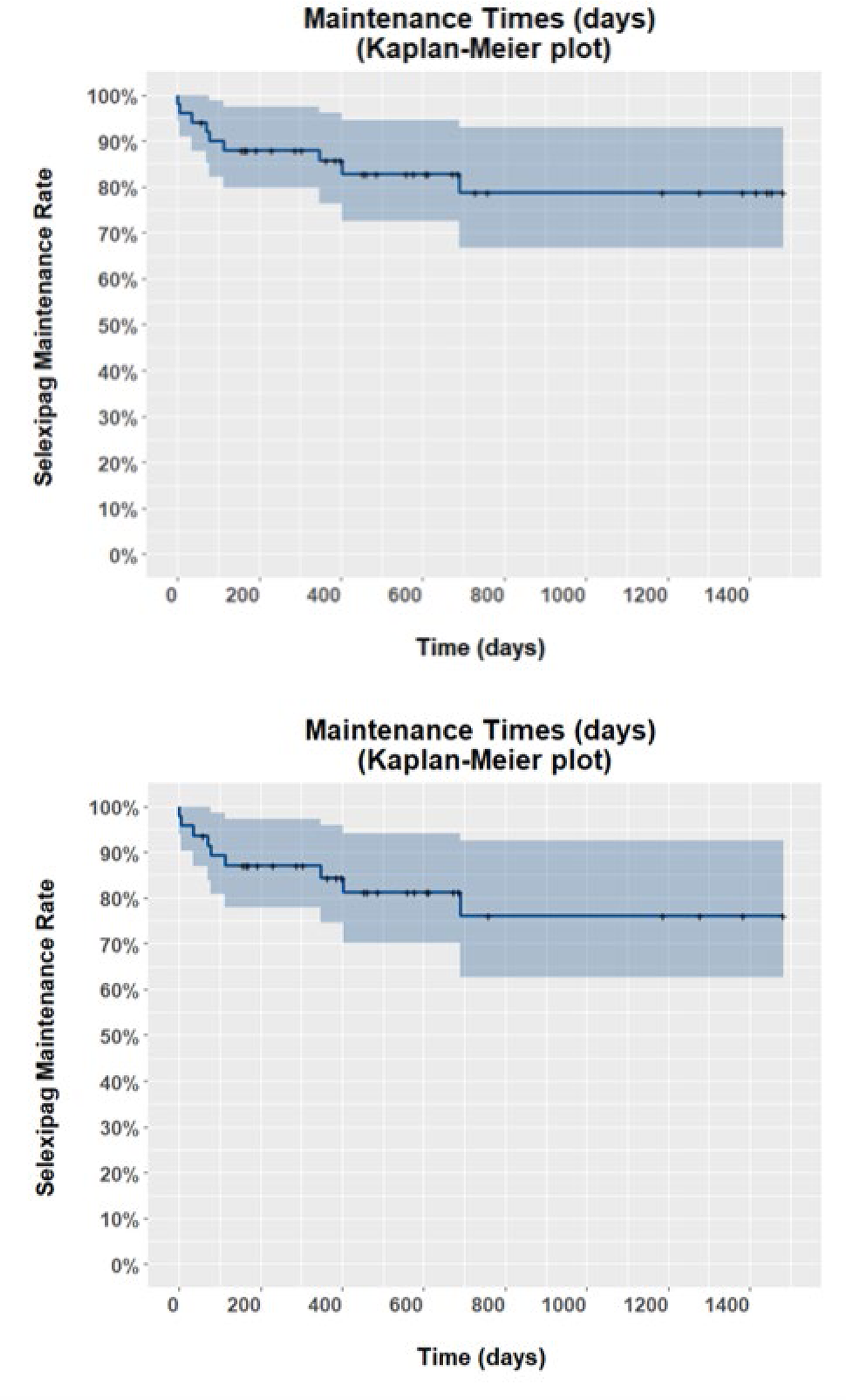
Results: A total of 51 pts were included. Characteristics at baseline (visit closest to selexipag initiation) for prevalent users (n=4), incident users (n=47) and the overall cohort are summarized in Table 1 . Risk assessment was available for 25 (49%) pts, and it was high-risk in 4 (8%) pts, intermediate-high in 12 (24%) pts, intermediate-low in 4 (8%) pts and low in 5 (10%) pts. Most pts (18, 72%) were NYHA class III. DUCAS score at baseline was 0 in 46 pts, and 2, 4 and 5 in 1 pt each. Persistency curves of selexipag treatment in the overall population and incident pts are presented in Figure 1 . Follow-up visit was available for 20 incident pts at 12 ± 3 months. 6MWT follow-up data were available for 5 pts; it was unchanged in 2 (10%) pts and improved in 3 (15%) pts; NYHA functional class was available for 11 pts; it was unchanged in 9 (45%) pts, improved in 1 pt (5%) and worsened in 1 pt (5%); risk assessment as available for 13 pts, and it was unchanged in 8 (40%) pts, improved in 2 (10%) pts and worsened in 3 (15%) pts; number of DUs was available for 11 pts and it was unchanged in 9 (45%) pts and improved in 2 (10%) pts.
Conclusions: In this real-world study in SSc-PAH pts, selexipag showed a high and sustained long-term treatment persistency, both in the overall population and among incident users. Treatment retention remained close to 80% beyond two years of follow-up, supporting the feasibility and tolerability of selexipag in routine clinical practice in a complex SSc population. Despite limitations due to missing data and the small number of pts with complete longitudinal assessments, clinical outcomes at 12 months for most patients remained stable, considering that 32% of pts were at an advanced stage of disease (intermediate-high or high risk) at baseline. Moreover, DU burden was largely stable.
| Characteristic | Overall
| Incident
| Prevalent
|
|---|---|---|---|
| Age (years) | |||
| Mean (SD) | 67 (12) | 68 (12) | 67 (14) |
| Median, [Min, Max] | 68, [33, 91] | 69, [33, 91] | 63, [55, 85] |
| Sex | |||
| Male | 7 (14%) | 6 (13%) | 1 (25%) |
| Height (cm) | |||
| Mean (SD) | 163 (9) | 163 (9) | 165 (8) |
| Missing | 8 [16%] | 7 [15%] | 1 [25%] |
| Body Weight (kg) | |||
| Mean (SD) | 71 (14) | 71 (14) | NA (NA) |
| Median, [Min, Max] | 75, [48, 92] | 75, [48, 92] | NA, [Inf, -Inf] |
| Missing | 28 [55%] | 24 [51%] | 4 [100%] |
| Race | |||
| Any other white | 35 (69%) | 33 (70%) | 2 (50%) |
| Black Caribbeans | 1 (2.0%) | 1 (2.1%) | 0 (0%) |
| Hispanic White | 1 (2.0%) | 1 (2.1%) | 0 (0%) |
| South Asians | 1 (2.0%) | 1 (2.1%) | 0 (0%) |
| Unknown | 1 (2.0%) | 1 (2.1%) | 0 (0%) |
| White | 12 (24%) | 10 (21%) | 2 (50%) |
| Age at Selexipag Start | |||
| Mean (SD) | 63 (11) | 63 (11) | 61 (12) |
| Median, [Min, Max] | 63, [32, 84] | 64, [32, 84] | 58, [51, 77] |
| Time to Selexipag (months) | |||
| Mean (SD) | 44 (64) | 39 (44) | 99 (174) |
| Median, [Min, Max] | 19, [0, 361] | 19, [0, 153] | 16, [5, 361] |
| Missing | 4 [7.8%] | 4 [8.5%] | 0 [0%] |
| Subsets of SSc | |||
| Diffuse cutaneous SSc | 8 (16%) | 7 (15%) | 1 (25%) |
| Limited cutaneous SSc | 38 (75%) | 35 (74%) | 3 (75%) |
| Sine scleroderma | 4 (7.8%) | 4 (8.5%) | 0 (0%) |
| Unknown | 1 (2.0%) | 1 (2.1%) | 0 (0%) |
| Autoantibodies Profile | |||
| Anti-centromere | 24 (47%) | 22 (47%) | 2 (50%) |
| Anti-Scl70 | 6 (12%) | 6 (13%) | 0 (0%) |
| Anti RNA polymerase III | 1 (2.0%) | 1 (2.1%) | 0 (0%) |
| Unknown | 20 (39%) | 18 (38%) | 2 (50%) |
| 6 Minute Walk Distance Test (m) | |||
| Mean (SD) | 300.41 (121.47) | 300.41 (121.47) | NA (NA) |
| Median, [Min, Max] | 324.00, [45.00, 501.00] | 324.00, [45.00, 501.00] | NA, [Inf, -Inf] |
| Missing | 34 [67%] | 30 [64%] | 4 [100%] |
| NYHA functional class | |||
| I | 1 (4.0%) | 1 (4.0%) | 0 (NA%) |
| II | 5 (20%) | 5 (20%) | 0 (NA%) |
| III | 18 (72%) | 18 (72%) | 0 (NA%) |
| Unknown | 1 (4.0%) | 1 (4.0%) | 0 (NA%) |
| Missing | 26 [51%] | 22 [47%] | 4 [100%] |
| NT-proBNP (pg/ml) | |||
| Mean (SD) | 1,638 (2,573) | 1,638 (2,573) | NA (NA) |
| Median, [Min, Max] | 790, [7, 11,292] | 790, [7, 11,292] | NA, [Inf, -Inf] |
| Missing | 28 [55%] | 24 [51%] | 4 [100%] |
| BNP (pg/ml) | |||
| Mean (SD) | 128.00 (106.35) | 128.00 (106.35) | NA (NA) |
| Median, [Min, Max] | 112.50, [22.00, 265.00] | 112.50, [22.00, 265.00] | NA, [Inf, -Inf] |
| Missing | 47 [92%] | 43 [91%] | 4 [100%] |
| Risk assessment | |||
| High-Risk | 4 (7.8%) | 4 (8.5%) | 0 (0%) |
| Intermediate High-Risk | 12 (24%) | 11 (23%) | 1 (25%) |
| Intermediate Low-Risk | 4 (7.8%) | 4 (8.5%) | 0 (0%) |
| Low-Risk | 5 (9.8%) | 5 (11%) | 0 (0%) |
| Unknown | 26 (51%) | 23 (49%) | 3 (75%) |
A. Overall population (N=51) and B. Incident patients (N=47)
REFERENCES: NIL.
Acknowledgments: NIL.
Disclosure of Interests: Corrado Campochiaro Speaker bureau from boeringher Johnson & Johnson, Maria Grazia Lazzaroni: None declared, Liala Moschetti: None declared, Giacomo De Luca: None declared, Silvia Bellando-Randone: None declared, Elisabetta Zanatta fees for consultancy speaking and lectures from Boehringer Ingelheim and Janssen., Gianluca Moroncini: None declared, Maria De Santis: None declared, Michael Hughes Speaker fees from Janssen, outside of the submitted work, Research funding, Juan Jose Alegre Sancho: None declared, Gonçalo Boleto: None declared, Paolo Airò: None declared, Francesco Del Galdo: None declared, Masataka Kuwana: None declared, Marie-Elise Truchetet consultant for Boehringer Ingelheim, AbbVie, Johnson and Johnson, Lilly, UCB. Congress Support from AbbVie, Johnson and johnson, Marco Matucci-Cerinic: None declared, Madelon Vonk Received speaker fees from Boehringer Ingelheim, Janssen Pharmaceutical Companies of Johnson & Johnson, MSD and Novartis, Received research grants from Boehringer Ingelheim, Ferrer and Galapagos, received consulting fees from Boehringer Ingelheim and Janssen Pharmaceutical Companies of Johnson & Johnson; treasurer of EUSTAR and steering committee member of the ERN ReCONNET