fetching data ... 
Background: Rheumatic polymyalgia (PMR) is more commonly observed in individuals over the age of 50, who may have a higher prevalence of osteoporosis, diabetes, cardiovascular diseases, and other chronic conditions. Currently, glucocorticoids are the primary treatment for PMR, but they can lead to various side effects, and recurrence is common during steroid tapering. Our previous 24-week study confirmed the effective treatment of PMR patients with tofacitinib. Given the relatively slow efficacy of tofacitinib, early adjunctive therapy with NSAIDs is needed. To address this, we are planning an open-label 52-week randomized controlled trial (NCT06172361).
Objectives: This study aims to assess the use tofacitinib in combination with glucocorticoids to induce rapid improvement, followed by rapid tapering of steroids and slow tapering of tofacitinib. The objective is to observe the efficacy and safety of this regimen for PMR, providing a new treatment option for clinical use.
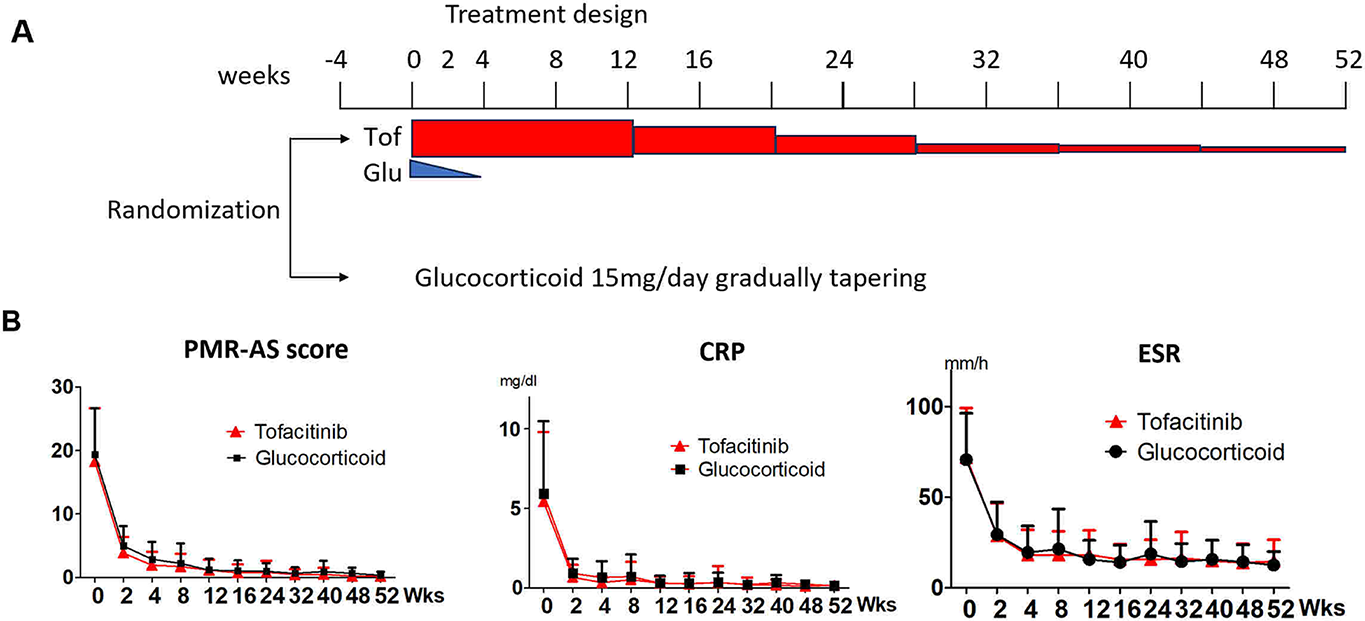
Methods: PMR patients who fulfilled the 1982 Chuang criteria or 2012ACR/EULAR criteria for PMR; They did not receive any glucocorticoids or biological agents during the 2 weeks period that preceded their inclusion in the study; Patients with high activity (PMR-AS>10) plus with ESR>20mm/h or CRP >50mg/L. The enrolled patients were randomized to treatment group (prednisone 15mg qd, withdrawal within 4 weeks+tofacitinib 5mg bid gradually tapering) or control group: prednisone 15mg qd (or equivalent dose of methylprednisolone), gradually tapering (Figure 1A). All PMR patients underwent clinical and laboratory examinations at 0、2、4、8、12、16、24、32、40、48、and 52 weeks, and PMR-AS activity disease scores were calculated. The primary endpoint was the proportion of patients with PMR-AS ≤10 at weeks 52. Secondary endpoints: PMR-AS score, c-reactive protein (CRP), and erythrocyte sedimentation rate (ESR) at weeks 24 and 52. Safety issues were recorded.
Results: We recruited PMR patients from the First Affiliated Hospital, Zhejiang University School of Medicine, from January 2024 to January 2026. 104 patients with PMR were enrolled and randomized (1/1) to treatment group and control group. 52 patients (38 female, 14 male, age 68.7 ± 8.3) were enrolled in treatment group. Among the participants, 49 subjects completed the 52-week follow-up, and 3 subjects dropped out. 52 patients (39 female, 13 male, age 67.5 ± 9.2) were enrolled in control group. Among them, 49 subjects completed 52-week follow-up, 3 subjects dropped out (Table 1). All patients who finished 52-week follow-up in two groups had all PMR-AS <10. PMR-AS, CRP, and ESR were all significantly decreased in both groups (Figure 1B). At weeks 24 and 52, PMR-AS score, CRP, and ESR levels were all comparable in treatment and control groups. The doses of tofacitinib are 3.98±2.38 mg daily at Weeks 52. The doses of prednisone are 3.89±2.83 mg daily at Weeks 52. No severe adverse events were observed in both group. Interestingly, the proportion of new-onset diabetes in treatment group was significantly lower than that in control group ( p = 0.0118) during the follow-up period. The proportion of new-onset hyperglycemia in the treatment group showed a tendency to be lower than that in control group, but there was no statistical difference (Table 1).
Conclusions: The results revealed that tofacitinib in combination with rapid tapering of steroids provided a rapid improvement and maintained a good remission. The dose of tofacitinib were decreased to low level at weeks 52. Tofacitinib showed a better safety profile and a significantly favorable impact on blood glucose levels than glucocorticoids.
Induction and tapering therapy with tofacitinib and glucocorticoids demonstrated good efficacy in patients with PMR
The characteristics of PMR patients
| Items | Tof+GCs: Treatment group (n=52) | GCs: control group (n=52) | P value |
|---|---|---|---|
| Gender | 38 female, 14 male | 39 female, 13 male | 0.9611 |
| Age (years) | 68.7 ± 8.3 | 67.5 ± 9.2 | 0.6118 |
| Follow-up | 49 cases completed 52-week follow-up, 3 cases were lost | 49 cases completed 52-week follow-up, 3 cases were lost | N/A |
| PMR-AS scores (baseline) | 18.5 ± 8.0 | 19.2 ± 7.1 | 0.2923 |
| CRP (mg/dl) (baseline) | 5.42 ± 4.33 | 5.91 ± 4.48 | 0.4017 |
| ESR (mm/h) (baseline) | 71.7 ± 27.1 | 70.3 ± 25.7 | 0.7377 |
| Diabetes (Baseline) | 7/52 | 9/52 | 0.5921 |
| New-onset Diabetes (follow-up) | 1/44 | 8/41 | 0.0118* |
| Hyperglycemia (baseline) | 6/52 | 7/52 | 0.798 |
| New-onset hyperglycemia (follow-up) | 10/43 | 16/42 | 0.142 |
| Infection | 5/52 | 5/52 | 0.9949 |
| Death | 0 | 0 | N/A |
| Respiratory infections | 0/52 | 1/52 | 0.567 |
| Herpes zoster | 4/52 | 1/52 | 0.407 |
| Urinary infection | 1/52 | 1/52 | 0.988 |
REFERENCES: [1] Devauchelle-Pensec V, Carvajal-Alegria G, Dernis E, Richez C, Truchetet ME, Wendling D, et al. Effect of Tocilizumab on Disease Activity in Patients With Active Polymyalgia Rheumatica Receiving Glucocorticoid Therapy: A Randomized Clinical Trial. JAMA. 2022;328(11):1053-62.
[2] Strand V, Msihid J, Sloane J, Nivens MC, Chao J, Giannelou A, et al. Sarilumab in relapsing polymyalgia rheumatica: patient-reported outcomes from a phase 3, double-blind, randomised controlled trial. Lancet Rheumatol. 2025;7(8):e544-e53.
[3] Spiera RF, Unizony S, Warrington KJ, Sloane J, Giannelou A, Nivens MC, et al. Sarilumab for Relapse of Polymyalgia Rheumatica during Glucocorticoid Taper. N Engl J Med. 2023;389(14):1263-72.
[4] Saraux A, Carvajal Alegria G, Dernis E, Roux C, Richez C, Tison A, et al. Baricitinib in early polymyalgia rheumatica (BACHELOR): a randomised, double-blind, placebo-controlled, parallel-group trial. Lancet Rheumatol. 2025;7(4):e233-e42.
[5] Ma X, Yang F, Wu J, Xu B, Jiang M, Sun Y, et al. Efficacy and Safety of Tofacitinib in Patients with Polymyalgia Rheumatica (EAST PMR): An open-label randomized controlled trial. PLoS Med. 2023;20(6):e1004249.
Acknowledgments: NIL.
Disclosure of Interests: None declared.