fetching data ... 
Background: Advances in vascular imaging have improved the diagnosis of giant cell arteritis (GCA), including large-vessel vasculitis (LVV). Treatment strategies have also evolved with targeted therapies such as tocilizumab (TCZ), as the GiACTA trial [1] showed sustained glucocorticoid (GC)-free remission with TCZ. Based on this evidence, international guidelines recommend TCZ as a standard option. However, in real-world practice, the optimal timing for TCZ initiation remains unclear. Traditionally reserved for refractory or relapsing cases, TCZ is increasingly considered for upfront use. Determining whether early TCZ can accelerate GC tapering and improve outcomes is a pressing clinical question. This study aimed to assess the impact of upfront TCZ initiation on GC tapering and treatment outcomes in real-world settings.
Objectives: To compare longitudinal GC tapering outcomes and clinical relapse rates between two treatment eras; an era of step-up TCZ use and a recent era of proactive upfront TCZ strategy.
Methods: This single-center retrospective study analyzed consecutive patients with newly diagnosed GCA treated between 2018 and 2025. The study period was chronologically divided into two eras to capture the strategic shift in practice: the Early Era (2018–2021), corresponding to a period of standard GC tapering with step-up TCZ use, and the Late Era (2022–2025), reflecting the adaptation of a proactive upfront TCZ strategy. Longitudinal GC tapering trajectories (expressed as prednisolone [PSL] equivalent doses) over the first 6 months were assessed using a linear mixed-effects model (LMM) with random intercepts and slopes, evaluating the interaction between Era and time. Secondary outcomes included the estimated cumulative GC dose over 6 months and achievement rates of stringent GC targets (≤7.5 and ≤5 mg/day) at Month 6. Clinical relapse rates were also compared between eras; relapse was defined as disease recurrence requiring GC dose escalation determined by the attending physician. Unfavorable clinical events were defined as death, serious infection requiring hospitalization, major adverse cardiovascular events (MACE), gastrointestinal events, fragility fractures, and herpes zoster. Multivariable linear regression analyses were performed to determine the independent effect of treatment era on GC dose at Month 6, adjusting for age, sex, cranial phenotype (cranial vs LVV), baseline CRP, and initial GC dose. To verify the robustness of our findings and capture the continuous evolution of treatment effects, a sensitivity analysis using a three-period trend model (2018–2020, 2021–2022, 2023–2025) was performed to assess stepwise temporal improvement.
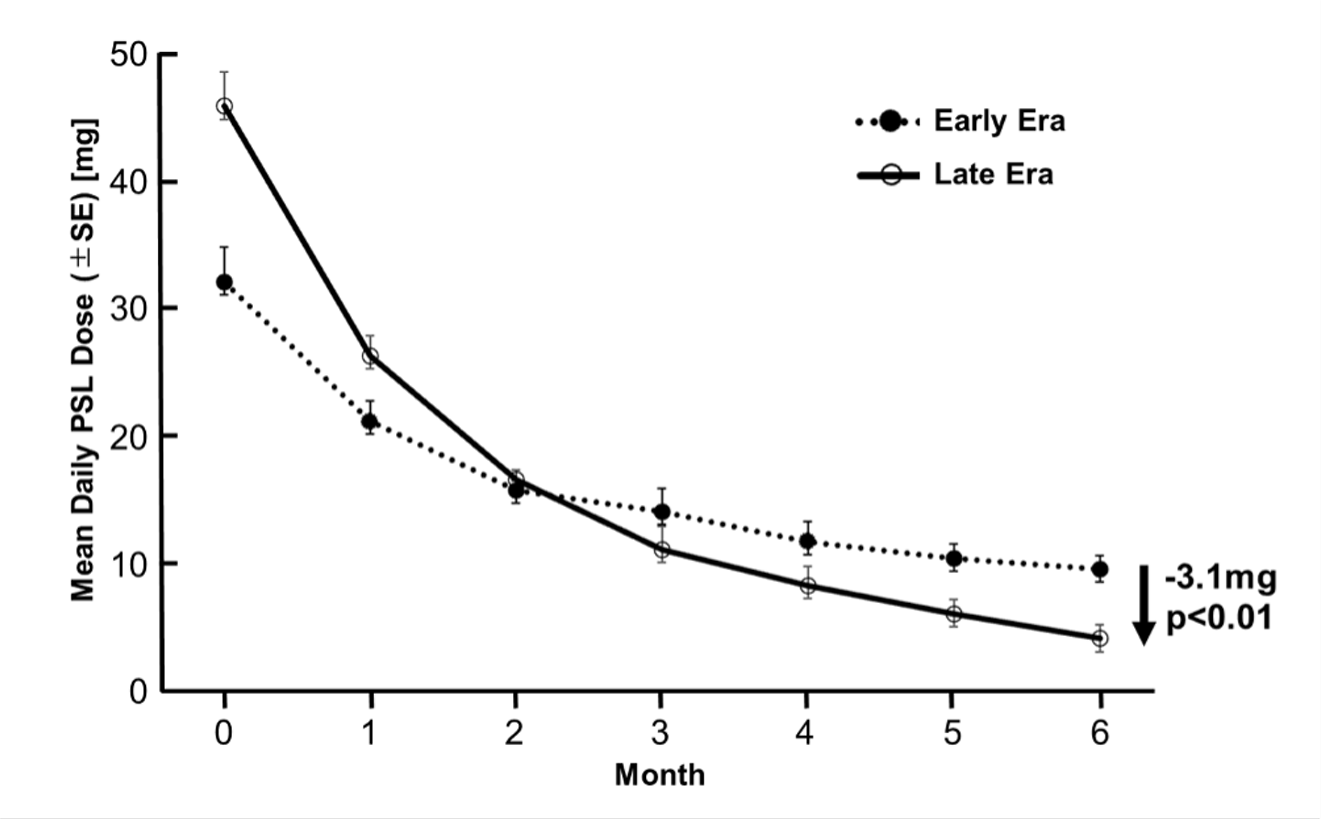
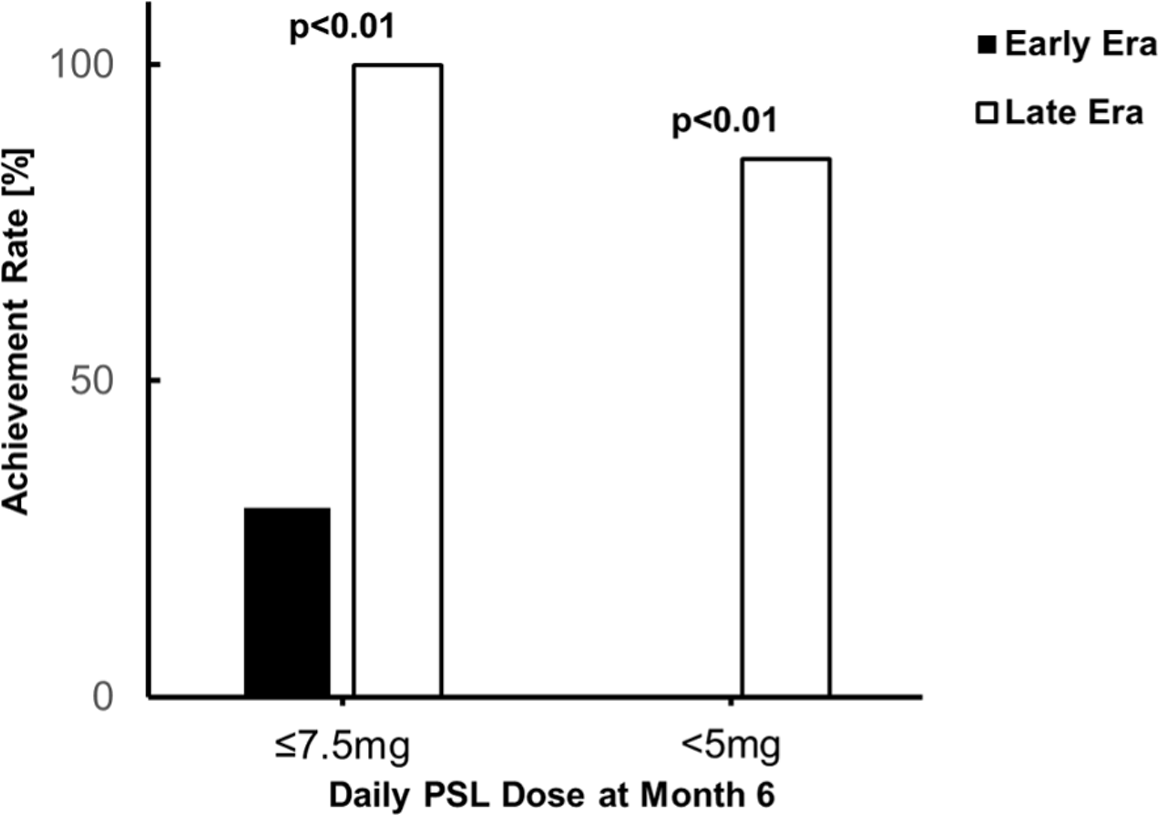
Results: A total of 31 patients were included (Early Era: n=12; Late Era: n=19). Baseline characteristics were comparable between groups, including female proportion (83% vs 63%, p=0.42), median age (75.5 vs 73.0 years, p=0.39), and median CRP (6.1 vs 6.2 mg/dL, p=0.69). However, the Late Era cohort presented with a higher prevalence of LVV (75.0% vs 89.5%, p=0.57) and required significantly higher initial median GC doses (30.0 vs 50.0 mg/day, p<0.01). TCZ use increased significantly from 41.7% in the Early Era to 94.4% in the Late Era (p<0.01), with a median time from diagnosis to TCZ initiation of 40.0 days in the Early Era and 21.0 days in the Late Era (p=0.61). In longitudinal analysis of daily GC dose (Figure 1), the LMM showed that the Late Era had a significantly higher initial intercept (Estimate: +9.9 mg/day, p<0.01) but a significantly steeper tapering slope compared to the Early Era (Era×Time Interaction: -3.1 mg/day per month, p<0.01). Despite the significantly higher initial doses, the estimated cumulative GC dose over 6 months was comparable between groups (Median: 3,060 vs 3,225 mg, p=0.34). At Month 6, the Late Era showed significantly higher achievement rates for stringent targets compared to the Early Era: GC dose ≤7.5 mg/day (30% vs 100%, p<0.01) and ≤5 mg/day (0% vs 85%, p<0.01) (Figure 2). Multivariable regression confirmed the Late Era was independently associated with lower GC dose at Month 6 (Estimate: -4.90 mg/day, p<0.01). Sensitivity analysis using the three-period model further confirmed a stepwise reduction in the mean GC dose at Month 6 (2018–2020: 8.8 mg/day, 2021–2022: 6.9 mg/day, and 2023–2025: 4.3 mg/day; p for trend <0.01). Regarding clinical outcomes, relapse was observed in 8.3% (1/12) of the Early Era patients (median follow-up: 1,638 days) and 0% (0/19) of the Late Era patients (median follow-up: 369 days). Overall incidence of unfavorable clinical events was found in 33.3% of the Early Era patients and 21.1% of the Late Era patients (p=0.73), including death (8.3% vs 0%, p=0.39), serious infection (8.3% vs 0%, p=0.39), MACE (8.3% vs 10.5%, p=1.00), gastrointestinal events (16.7% vs 0%, p=0.14), fragility fractures (0% vs 5.3%, p=1.00), and herpes zoster (0% vs 5.3%, p=1.00), respectively.
Conclusions: An upfront TCZ strategy was associated with significantly steeper GC tapering and superior achievement of stringent low-dose targets (≤5 mg/day) at Month 6, despite higher initial GC requirements in Late era. Furthermore, no clinical relapses were observed in the Late Era, and the adverse events were comparable between the two Eras. These real-world data demonstrate that rapid tapering to low-dose GC is achievable with an upfront TCZ strategy, yielding treatment results comparable to conventional therapy.
Daily Glucocorticoid Dose Trajectories.
The time course of mean daily prednisolone (PSL) equivalent doses in the Early Era (dotted line) and Late Era (solid line). Error bars represent standard errors (SE).
Achievement Rates of Stringent Glucocorticoid Targets at Month 6.
Comparison of the proportion of patients achieving daily GC doses of ≤ 7.5 mg and ≤ 5 mg at Month 6 between the Early Era (black bar) and Late Era (white bars).
REFERENCES: [1] Stone JH, et al. N Engl J Med 2017; 377: 317-328.
Acknowledgments: NIL.
Disclosure of Interests: None declared.