fetching data ... 
Background: The prognosis of rheumatoid arthritis (RA) improves if treatment is initiated within three months of symptom onset, often referred to as ‘a window of opportunity [1]. However, less than one third of patients are assessed by a rheumatologist within the recommended timeframe [2]. Overall, the time to initiate treatment in RA has declined over the last few years, due to improvements within the healthcare system, such as new approaches to diagnosis, and clinical awareness [3]. However, patient factors are often overlooked, and the time from symptom onset to seeking care from a general practitioner (GP) remains a major contributor to the overall time to treatment [4]. In recent years, socioeconomic status (SES) has become an important factor in health-related outcomes and behaviour, with studies suggesting RA patients with low SES experience worse disease activity, quality of life, disability, as well as physical and mental health [5]. Understanding this association is crucial for addressing health inequalities, as socioeconomic disparities may contribute to delayed diagnosis and worse disease outcomes.
Objectives: To examine the association between SES and time to help-seeking in people newly diagnosed with RA.
Methods: Data on incident RA were obtained from the Danish Rheumatology Database (DANBIO), and patients’ self-reported time from RA symptom onset to first GP contact were collected via questionnaires. Responses were linked to Danish National Registries via Statistics Denmark, for SES information (exposure). This included education, wealth, cohabitation status, and occupation. The outcome of interest was the self-reported time from RA symptom onset to seeking care from a GP. We calculated the median duration from symptom onset to first GP contact (patient interval) overall and by SES markers, with corresponding interquartile ranges (IQRs). The outcome was dichotomized into <3 months versus ≥3 months, and the association between SES and time to first general practitioner contact was analysed using multiple logistic regression models, presented as odds ratios (ORs) with 95% confidence intervals (CIs). The first model was adjusted for sex, age and comorbidity, and the second was additionally adjusted for clinical disease activity measures (C-reactive protein, tender- and swollen joints). Lastly, we investigated selection bias by comparing the SES characteristics of respondents and non-respondents to the questionnaire.
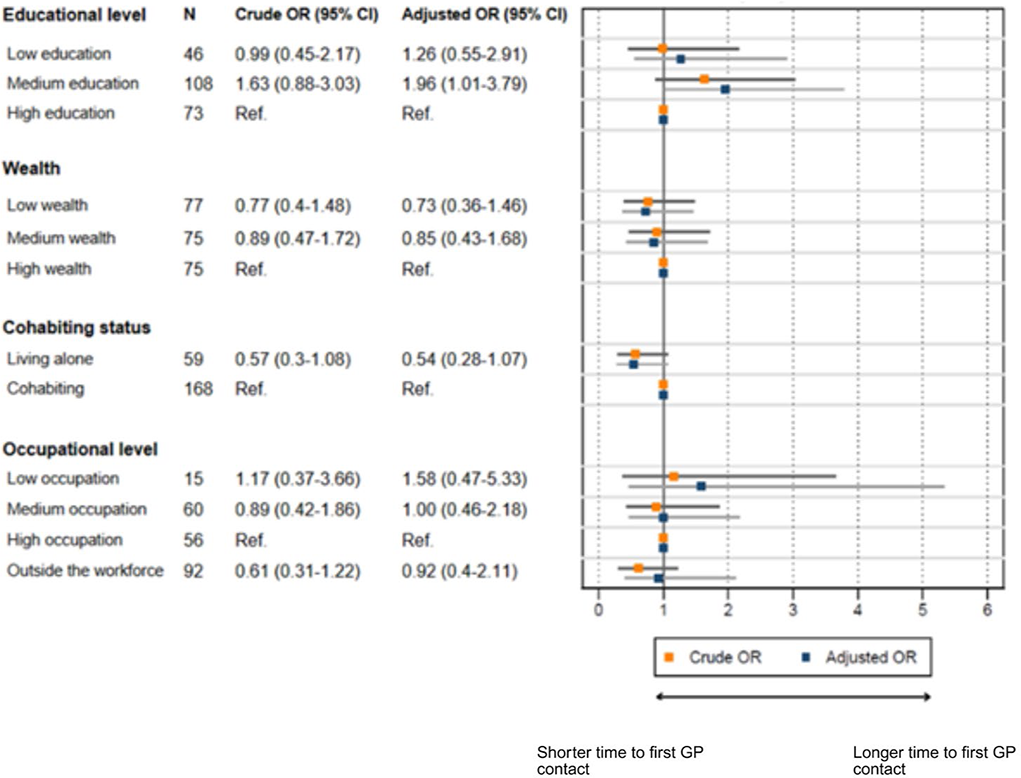
Results: A total of 404 patients were included. We excluded patients who had missing information on disease activity measures (C-reactive protein, tender- and swollen joints), which left us with 227 patients for analysis. The median time to first GP contact was 59 days (IQR 15–182). Medium educational level was associated with a longer time to first contact compared with high educational level (aOR 1.96, 95% CI 1.01–3.79), while low occupational status showed a tendency toward a longer time to first contact (aOR 1.58, 95% CI 0.47–5.33) (Figure 1). No consistent associations were observed for wealth or cohabitation. Longer times to first contact were observed among younger patients, patients without comorbidities, and patients with lower disease activity. Non-responders had significantly lower SES.
Conclusions: Educational level showed the strongest socioeconomic association with time to first GP contact. Findings from the non-response analysis indicate a potential overrepresentation of socially vulnerable patients among non-responders, highlighting the importance of equity considerations in early RA care pathways.
Logistic regression analyses of the association between markers of socioeconomic status and time to first general practitioner contact (<3 months vs ≥3 months). Crude and adjusted odds ratios are shown, with adjusted models controlling for sex, age, comorbidity, and disease activity measures, and presented with corresponding 95% confidence intervals.
REFERENCES: [1] van der Linden MP, le Cessie S, Raza K, van der Woude D, Knevel R, Huizinga TW, et al. Long-term impact of delay in assessment of patients with early arthritis. Arthritis Rheum 2010;62:3537-46.
[2] Raza K, Stack R, Kumar K, Filer A, Detert J, Bastian H, et al. Delays in assessment of patients with rheumatoid arthritis: variations across Europe. Ann Rheum Dis 2011;70:1822-5.
[3] Kumar K, Daley E, Carruthers DM, Situnayake D, Gordon C, Grindulis K, et al. Delay in presentation to primary care physicians is the main reason why patients with rheumatoid arthritis are seen late by rheumatologists. Rheumatology (Oxford) 2007;46:1438-40.
[4] Stack RJ, Nightingale P, Jinks C, Shaw K, Herron-Marx S, Horne R, et al. Delays between the onset of symptoms and first rheumatology consultation in patients with rheumatoid arthritis in the UK: an observational study. BMJ Open 2019;9:e024361.
[5] Zou Y, Cheung PP, Teoh LK, Chen C, Lahiri M. Sociodemographic factors as determinants of disease, disability and quality of life trajectories in early rheumatoid arthritis: A multi-ethnic inception cohort study. Int J Rheum Dis 2020;23:55-64.
Acknowledgments: NIL.
Disclosure of Interests: None declared.