fetching data ... 
Background: Oral health problems are common in rheumatoid arthritis (RA) and may contribute to frailty through systemic inflammation and downstream impacts on nutrition, mental health and sleep. However, the pathways connecting oral health and frailty in RA have not been well characterised in health-professional–relevant outcomes and care planning.
Objectives: To examine the association between oral health and frailty in RA and to quantify direct and indirect pathways via inflammation (CRP), nutritional status, depressive symptoms and sleep quality, using patient-reported outcome measures (PROMs) and clinically actionable mediators.
Methods: In this observational study, 318 patients with RA were recruited (September 2024–September 2025). Oral health was assessed using the Oral Health Assessment Tool (OHAT) and the Oral Health Impact Profile-14 (OHIP-14), alongside self-rated oral health and perceived chewing difficulty. Frailty was measured using the Tilburg Frailty Indicator (TFI). Nutritional status (MNA-SF), sleep quality (PSQI), depressive symptoms (PHQ-9) and inflammatory markers (CRP/ESR) were collected. Structural equation modelling (SEM) estimated standardized path coefficients and direct/indirect effects.
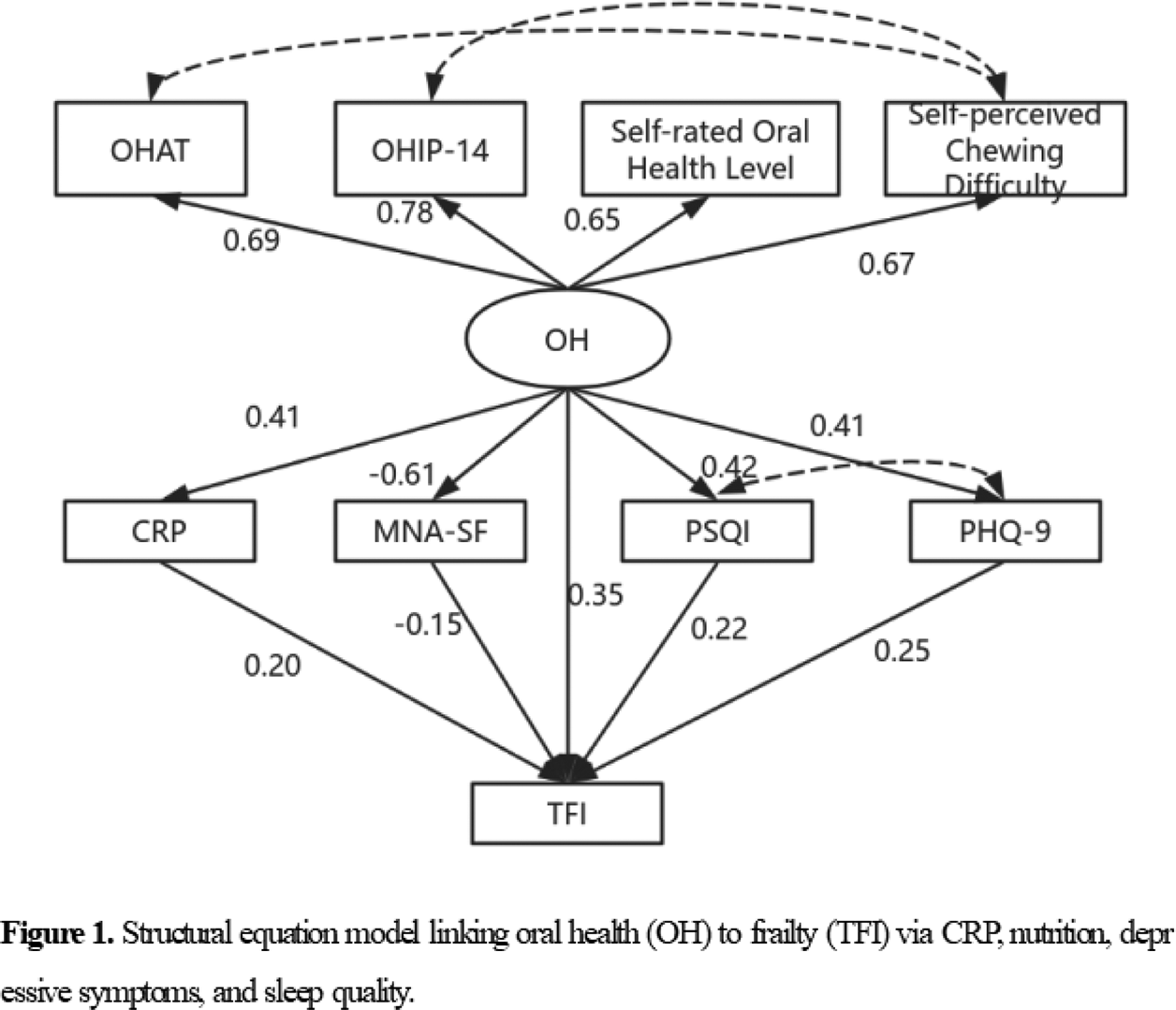
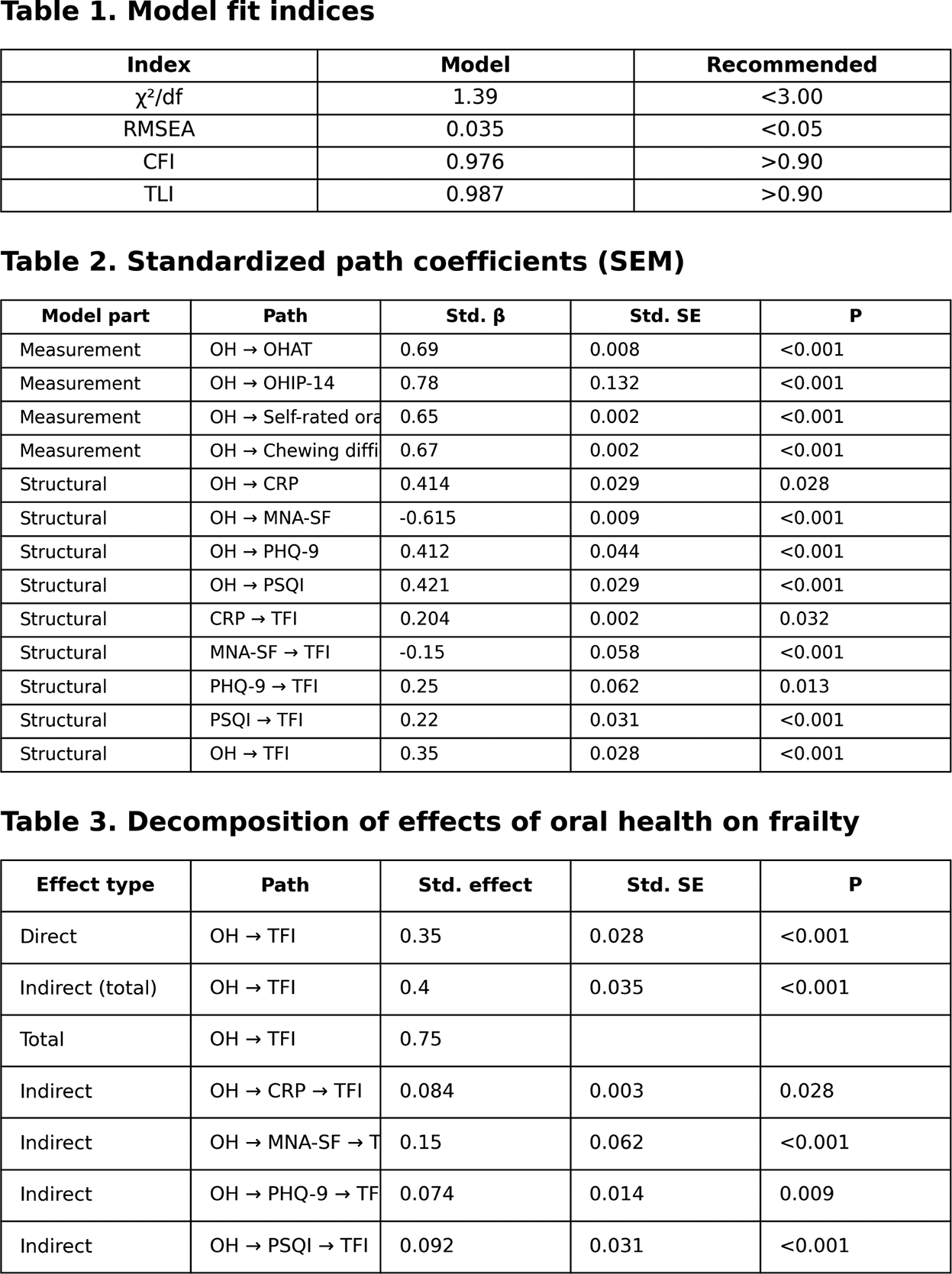
Results: Frailty was highly prevalent (76.1%). The SEM demonstrated good fit (χ 2 /df=1.390, RMSEA=0.035, CFI=0.976, TLI=0.987). The latent oral health construct (OH) was well indicated by OHAT (λ=0.690), OHIP-14 (λ=0.780), self-rated oral health (λ=0.650) and chewing difficulty (λ=0.670) (all P<0.001). Poorer oral health had a significant direct effect on frailty (OH→TFI: β=0.350, P<0.001) and significant indirect effects through clinically relevant pathways: OH→CRP→TFI (β=0.084, P=0.028), OH→MNA-SF→TFI (β=0.150, P<0.001), OH→PHQ-9→TFI (β=0.074, P=0.009) and OH→PSQI→TFI (β=0.092, P<0.001). The total indirect effect was 0.400 and the total effect was 0.750, indicating that mediation accounted for ~53.3% of the overall association.
Conclusions: In RA, poorer oral health is strongly associated with frailty, with more than half of the total effect mediated via CRP-related inflammation, malnutrition, depressive symptoms and poor sleep. These findings highlight PROM-informed, actionable targets for health professionals and support integrating routine oral screening with coordinated oral–nutrition–mental health–sleep management within multidisciplinary RA care to improve quality of care and mitigate frailty risk.
REFERENCES: [1] Tang SC, Jin L, Hu YQ, et al. The distribution of the frailty index among different arthritis patients and the association between the frailty index and mortality in rheumatoid arthritis patients among U.S. adults (results from NHANES 1999-2018). Aging Clin Exp Res . 2025;37(1):186.
[2] Brubeck HF, Riggles KE, Bass RS, et al. Evaluating the Longitudinal Association of Rheumatoid Arthritis Disease Activity with Phenotypic Frailty: Evidence for Secondary Frailty?. Arthritis Care Res (Hoboken ). Published online July 23, 2025.
[3] Salaffi F, Di Matteo A, Farah S, Di Carlo M. Inflammaging and Frailty in Immune-Mediated Rheumatic Diseases: How to Address and Score the Issue. Clin Rev Allergy Immunol . 2023;64(2):206-221.
Acknowledgments: NIL.
Disclosure of Interests: None declared.