fetching data ... 
Background: Non-communicable chronic diseases (NCDs) and rheumatic and musculoskeletal diseases (RMDs) constitute a major global health burden, with prevalence rising sharply in vulnerable populations. In the Global South, adverse social determinants, not only increase disease risk but also foster comorbidities between NCDs and RMDs, thereby worsening outcomes. Syndemic theory provides a framework to understand this negative synergy between diseases and social factors. In Mexico’s Maya-Yucatecan Indigenous communities, high rates of diabetes, hypertension, and RMDs intersect with barriers such as transportation gaps and cultural marginalization. Despite this syndemic burden, few interventions have been applied through the syndemic lens, emphasizing the necessity for context-specific, culturally grounded care models developed within these settings. This study focuses on the evaluation of a co-created intervention called Syndemic Care Model (SCM) using a Community-Based Participatory Research (CBPR) approach to address both clinical and structural drivers of health inequities in these populations.
Objectives: To evaluate the change in the syndemic of RMDs and NCDs in three Maya-Yucatecan Indigenous communities after the implementation of the SCM.
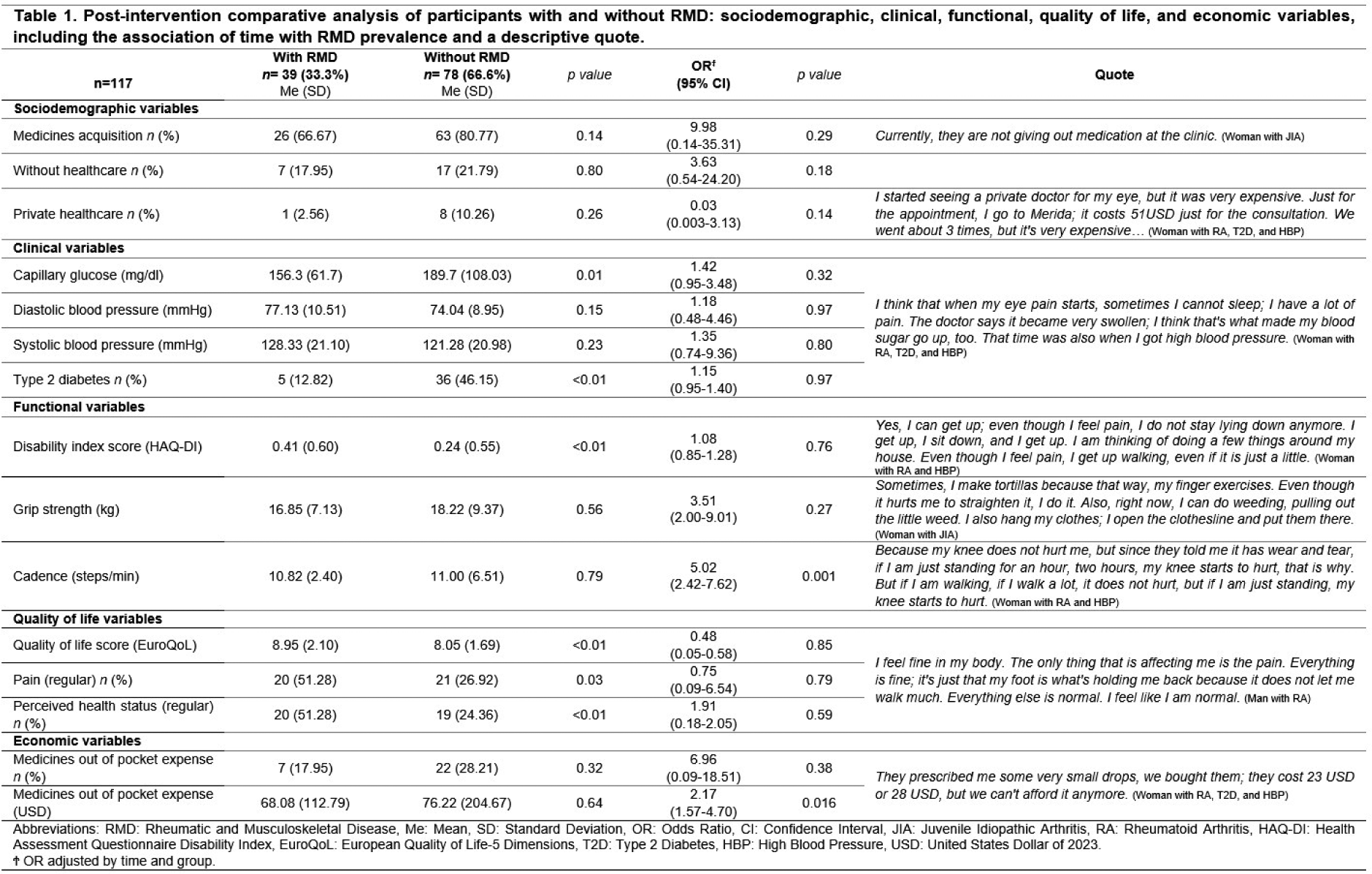
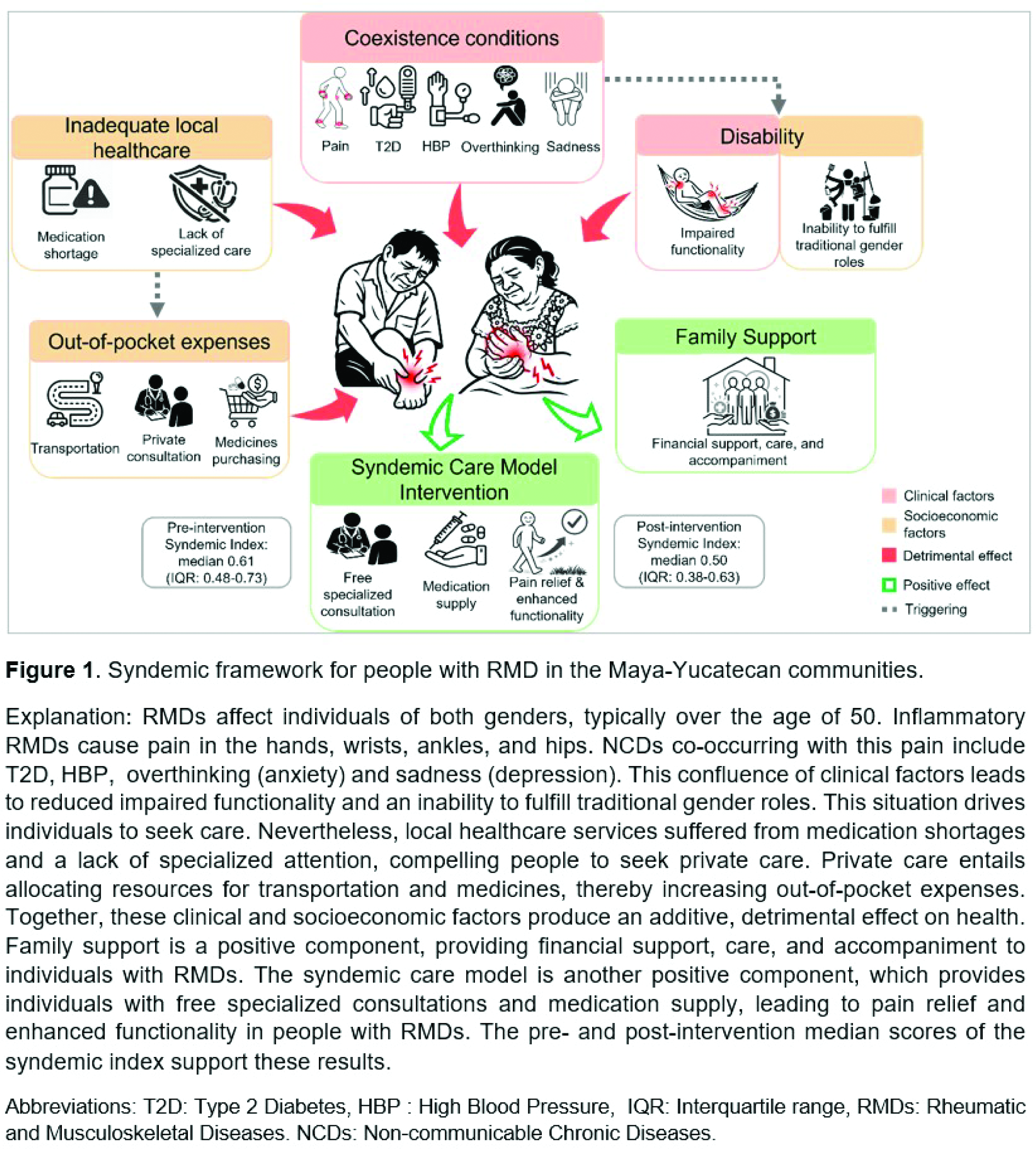
We employed a mixed-methods, convergent-parallel design, both quantitative (QUAN) and qualitative (QUAL); following different CBPR phases. The QUAN component included a before-after study (baseline and 6-month follow-up) including measurements of sociodemographic characteristics, comorbidities, HAQ-DI, EuroQoL-5D-3L, and functioning assessments. Participants with RMDs were matched 12 with non-RMD controls by age and sex. The QUAL component involved ethnographic fieldwork, including semi-structured interviews with RMD participants to understand lived syndemic experiences. Analysis included descriptive statistics, regression models for between-group differences over time, and multivariable logistic regression to identify RMD predictors. A continuous Syndemic Index was derived from key variables to assess change between baseline and 6-month follow-up after the intervention. Network analysis was used to visualize syndemic clustering across different groups. QUAL data were analyzed thematically and integrated with QUAN findings via triangulation in a sequential explanatory approach. Ethical approval was obtained, and all participants signed informed. Results: We included 39 RMD participants matched 1:2 with 78 controls (aged: mean 56 SD 13), most of them were women, and eight RMD patients were interviewed (age 24-81). Participating communities were characterized by type of basic utilities, lack of public transportation, and residents that engage in traditional gender roles. At baseline, individuals with RMDs demonstrated significantly worse functional performance, higher disability, greater pain intensity, and poorer self-rated health compared to controls. Out-of-pocket medication expenditures were also higher for the RMD group. QUAL interviews identified pain and disability as central theme, with the statement “The pain stops me from working” encapsulating the severe limitation on daily activities and traditional gender roles. Access to medications was lower for RMD participants (61.5%) compared to controls (80.7%), largely due to shortages at local public clinics, forcing recourse to private, expensive alternatives in distant urban centers. The SCM strengthened links with local healthcare systems and government to improve access to care, medicine, and transport. Free specialized consultations in communities and via telemedicine were offered, and established a basic wound care program with local women. Following the six-month SCM implementation, no significant differences were found between groups for most clinical and quality-of-life QUAN variables (Table 1). Changes were observed only in walking and increase in out-of-pocket medication expenses. However, QUAL findings supported patient-reported improvements. Participants described a transition from constant, debilitating pain to more manageable, occasional pain, alongside regained mobility for activities like walking and bending. The syndemic index was significantly higher in the syndemic group (RMD+NCD) at baseline (Median: 0.61, IQR: 0.48-0.73) compared to controls. Post-intervention, this index decreased (Median: 0.50, IQR: 0.38-0.63) while remaining stable for controls, indicating a reduction in cumulative burden. Network analysis visually confirmed this shift: at pre-intervention, RMD participants were clustered in high-burden network peripheries, but post-SCM, many migrated toward more central, moderate-burden clusters, aligning with QUAL reports of better function and pain control. Despite these gains, structural barriers persisted as dominant themes. Medication shortages, particularly for specialized RMD drugs, and the high transportation costs to referral centers continued to drive health insecurity and financial strain. Family support was identified as a mitigating factor. These results illustrate that the SCM yielded measurable reductions in syndemic burden and meaningful experiential improvements. Figure 1 summarizes QUAL results.
Conclusions: This study shows that a community-co-designed SCM reduced pain and improved walking mobility for individuals with RMDs in rural Maya communities. The development and application of a multidimensional syndemic index proved instrumental for measuring change and identifying subgroups for whom persistent structural barriers, including medication shortages, transportation costs, and fragmented referrals, limited improvements. These findings underscore that clinical interventions alone are insufficient without addressing systemic structural inequities. Consequently, a syndemic-informed, mixed-methods approach is essential for crafting effective, culturally grounded policies, and for monitoring progress toward reducing health disparities in marginalized populations.
REFERENCES: NIL.
Acknowledgments: NIL.
Disclosure of Interests: None declared.