fetching data ... 
Background: Menopause has been associated with an increased prevalence and severity of sexual dysfunction (SD); however, its impact on women with rheumatic musculoskeletal diseases (RMDs) has not been fully established [1]. In these patients, SD may occur before menopause due to disease-related factors such as chronic pain, fatigue, persistent inflammation, psychosocial comorbidity, and adverse effects of medications [2]. Therefore, it remains unclear whether menopause introduces changes in the specific domains affected, distinct from those driven by the primary rheumatic disease, or whether it intensifies sexual dysfunction already present before the menopausal transition.
Objectives: Describe sexual dysfunction by domains in premenopausal and postmenopausal women with RMDs, compare the severity between groups, and identify whether menopause modifies or intensifies the pattern of dysfunction in patients with pre-existing sexual dysfunction before menopause.
Methods: We conducted a cross-sectional study in adult women (>18 years) with at least one rheumatic disease at the outpatient rheumatology clinic at “Hospital Universitario Dr. José Eleuterio González”. The Arizona sexual experiences Scale (ASEX) questionnaire [3] was administered to evaluate sexual function; item 3a was excluded because it is intended only for men. SD was defined as a total score ≥19 points, at least one item with ≥5 points, or two items with ≥4 points. Patients without sexual activity or who did not reach a classification score for SD were excluded. Sociodemographic and clinical variables were obtained from medical records. According to normality assessed by the Shapiro–Wilk test, between group comparisons were performed using appropriate parametric or non-parametric tests.
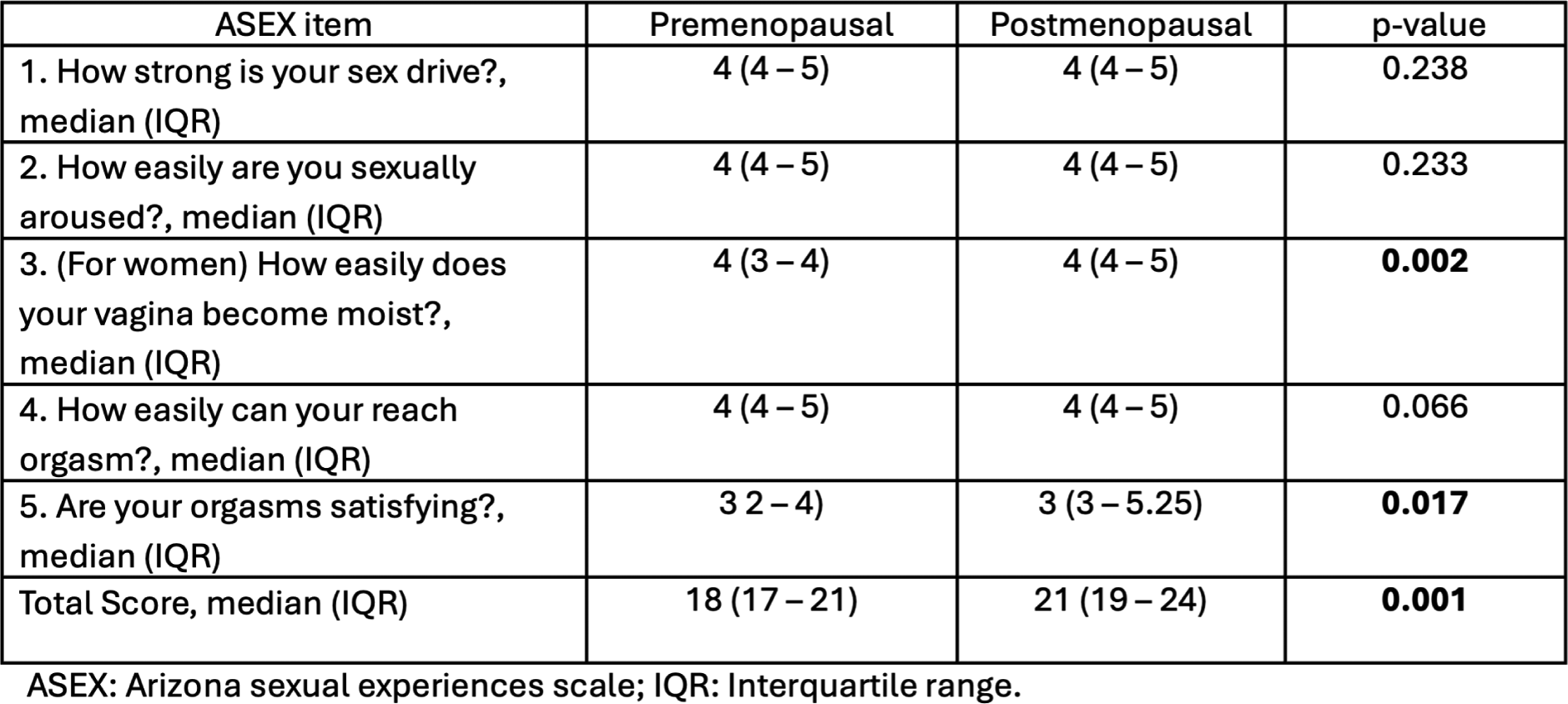
Results: A total of 491 women completed the questionnaire. Of these, 233 were sexually active. Among them, 153 met the ASEX criteria for SD and were included in the final analysis, resulting in a prevalence of 65.6%. The median age was 47 years (IQR 34–53), and the median disease duration was 4 years (IQR 1–8). Most participants were homemakers 94 (61.4%). Regarding educational level, 78 (51.6%) had a high level of education. The majority, 116 women (75.8%), were in a relationship. Most participants reported having children, 123 (80.4%), and antidepressant use within the past 12 months was identified in 26 (17.0%) (Table 1). Premenopzusal women showed a higher score in the domains of sexual drive, arousal, and ability to reach orgasm, all with a median score of 4 (IQR 4–5). Lubrication had a median of 4 (IQR 3–4), orgasmic satisfaction had a median of 3 (IQR 2–4), and the total score had a median of 18 (IQR 17–21). In postmenopausal women, the same domains (sexual drive, arousal, and ability to reach orgasm) showed similar values (4 [IQR 4–5]), with no significant differences in drive or arousal (p =.238 and p =.233, respectively), although a trend was observed in orgasmic ability ( p =.066 ). However, in postmenopausal women lubrication scores were higher, with a median of 4 (IQR 4–5) ( p =.002 ). Orgasmic satisfaction also showed higher values, with a median of 3 (IQR 3–5.25), which was statistically significant ( p =.017 ). The total ASEX score was significantly higher in postmenopausal women, with a median of 21 (IQR 19–24), compared with premenopausal women ( p =.001 ) (Table 2).
Conclusions: In both pre and postmenopausal groups, a similar pattern of SD was observed, with most items falling within the categories of “some weak” or “very weak,” even among premenopausal women. The only exception was orgasmic satisfaction, which remained within “somewhat satisfying” levels. However, the stratified analysis showed greater severity in postmenopausal women, particularly in lubrication and orgasmic satisfaction, along with a trend toward lower ease of reaching orgasm. This suggests that menopause does not alter the overall pre-existing pattern of sexual dysfunction but does intensify specific domains. Therefore, the menopausal transition represents a critical period to reduce the impact on sexual health in this population.
Table 1. Sociodemographic characteristics stratified by menopausal group.
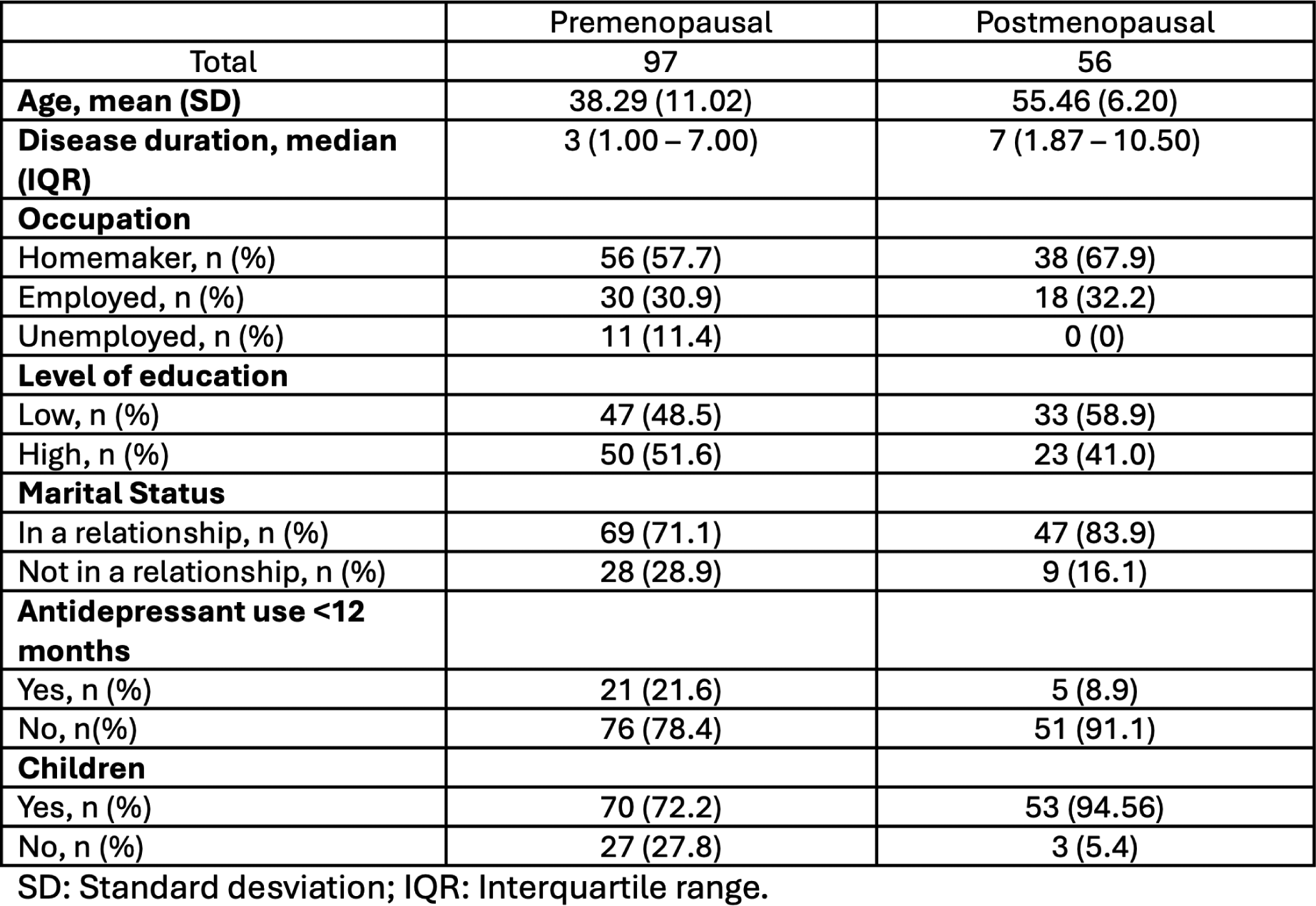
Table 2. Evaluation of sexual function according to menopausal group.
REFERENCES: [1] Østensen M. Sexual and reproductive health in rheumatic disease. Nature Reviews Rheumatology. 2017;13(8):485–93.
[2] Dag A, Ak T, Kaya E, Tulek Z, Poyraz BC, Ugurlu S, et al. Sexual dysfunction among female patients with rheumatic diseases. Rheumatology International. 2024;44(10):2099–109.
[3] McGahuey CA, Gelenberg AJ, Laukes CA, Moreno FA, Delgado PL, McKnight KM, et al. The Arizona Sexual Experiences Scale (ASEX): reliability and validity. J Sex Marital Ther. 2000;26(1):25–40.
Acknowledgments: NIL.
Disclosure of Interests: None declared.