fetching data ... 
Background: Physiotherapy is a core non-pharmacological intervention in the management of rheumatic and musculoskeletal diseases (RMD), contributing to functional recovery and quality of life [1]. Patients’ healthcare experiences may be influenced by social position, identity and care environments. Lesbian, gay, bisexual, transgender, queer, intersex, asexual and other sexual and gender minority (LGBTQIA+) individuals have been reported to encounter challenges within healthcare settings related to stigma, minority stress and heteronormative or cisnormative assumptions, which may influence access, communication, disclosure and perceived safety [2]. Despite increasing attention to diversity, equity and inclusion in healthcare, evidence on the experiences of LGBTQIA+ people within physiotherapy care remains limited, particularly in Italy. The 2025 ILGA-Europe Rainbow Map placed Italy 35th out of 42 European countries for legal and policy protections for LGBTQIA+ people, highlighting a context in which healthcare experiences may vary.
Objectives: To explore perceived safety and comfort, and perceived quality of care among LGBTQIA+ individuals receiving physiotherapy for RMD in Italy.
Methods: A mixed-methods study was conducted among LGBTQIA+ adults living in Italy who had accessed physiotherapy for any condition within the past two years. This abstract focuses on reporting the findings of the quantitative data collection through an anonymous online survey. The survey was informed by a literature review and co-developed with LGBTQIA+ patient research partners, healthcare professionals and researchers to ensure relevance and inclusivity. Collected variables included sociodemographic and clinical characteristics, care settings, disclosure of sexual orientation and gender identity, perceived comfort and safety, inclusivity of care environments, and overall perceptions of care quality. Data were analysed using descriptive statistics.
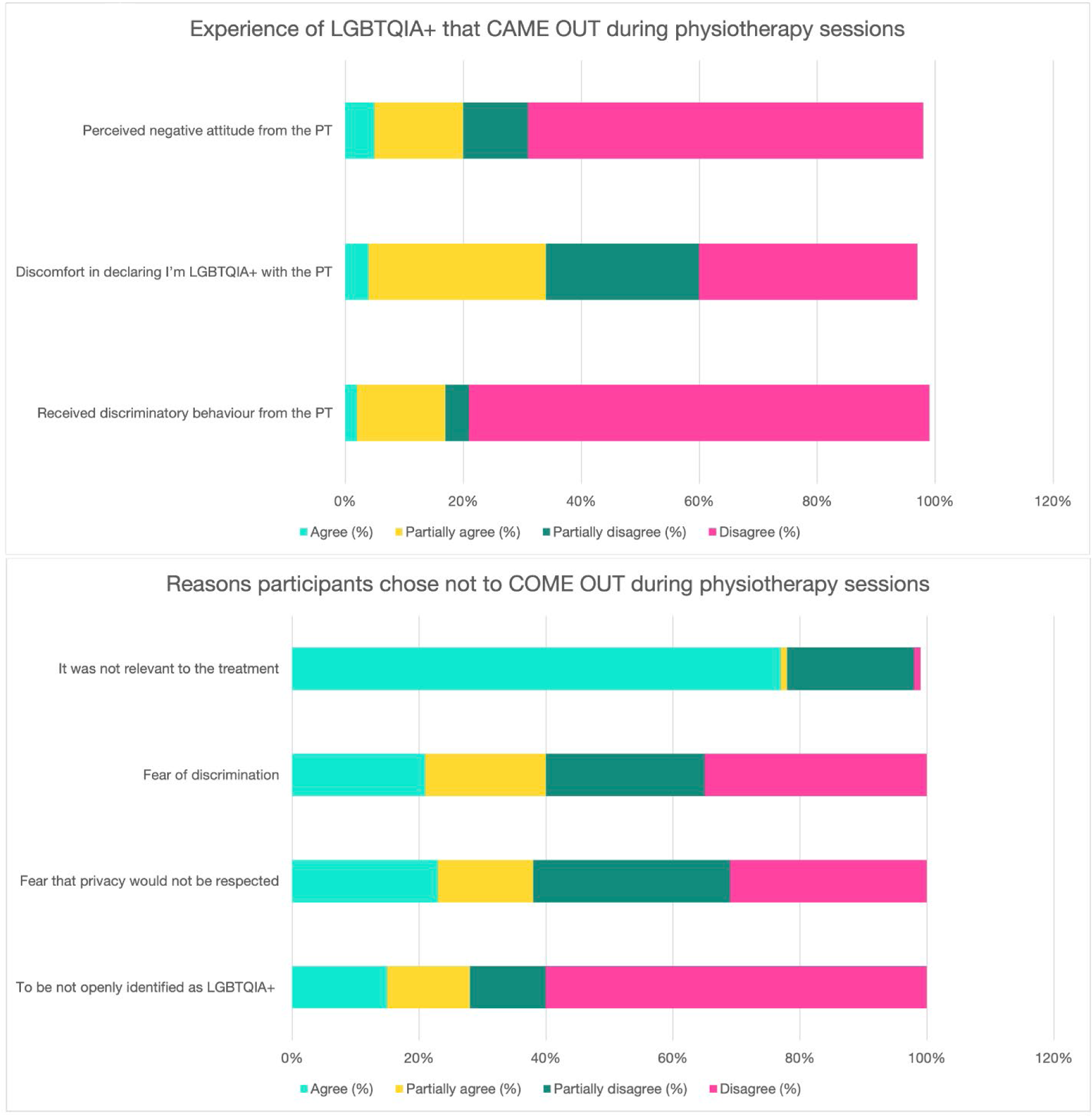
Results: Of the 288 responders, 120 LGBTQIA+ respondents (41.7%) who reported having accessed physiotherapy for RMD were included; the remaining respondents had accessed physiotherapy for other conditions. The sample comprised individuals with diverse gender identities (53.0% men, 33.0% women, 9.6% non-binary, 3.5% genderqueer and 0.9% transgender) and a range of sexual orientations, predominantly gay and lesbian (61.7%) and bisexual (21.7%). Physiotherapy care was most often accessed in private practices and outpatient services (63%). Levels of comfort during physiotherapy varied, with more than half of participants reporting low comfort in discussing their sexual orientation (53%) and 44% reporting low comfort in discussing their gender identity. Although overt discriminatory behaviours were rarely reported (6%), reduced comfort was frequently described, particularly in relation to interpersonal interactions and communication within the therapeutic context. Figure 1 shows limited inclusivity of physiotherapy environments based on the absence of specific features. Most participants indicated the lack of inclusive symbols (92%), non-discrimination statements (66%) and documentation attesting specific LGBTQIA+ training (74%). Only 1% reported the availability of non-binary or gender-diverse options in healthcare forms. Perceived awareness of LGBTQIA+-specific health needs among physiotherapists varied, with many participants reporting limited awareness. Disclosure of LGBTQIA+ identity during physiotherapy was reported by 36.5% of participants, while 63.5% reported non-disclosure. Among non-disclosing participants (n = 73), all reported at least partial agreement that non-disclosure was related to perceived irrelevance to therapy, concerns about privacy, and not being openly out (Figure 2). Although physiotherapy was generally perceived as beneficial for symptom management and physical function, perceived quality of care varied. Patterns of perceived safety, respectful communication and comfort within the therapeutic relationship were heterogeneous across participants. Those reporting higher levels of perceived safety and respectful communication also reported higher satisfaction with physiotherapy care, whereas participants reporting heteronormative or cisnormative assumptions reported lower perceived quality of care.
Conclusions: In this sample of LGBTQIA+ people with RMD, physiotherapy experiences appeared to be influenced less by overt discriminatory behaviours and more by interpersonal and contextual factors related to comfort, safety and disclosure. Despite low reported rates of explicit discrimination, discomfort in discussing sexual orientation and gender identity was common, suggesting a gap between non-discrimination and care environments perceived as sufficiently safe for open engagement. Non-disclosure was frequently reported and often described as not relevant to treatment; however, this pattern may also limit the visibility of negative experiences related to identity within physiotherapy settings. These findings should be interpreted in light of important limitations, including the small sample size and the use of an online, self-selected survey, which may limit representativeness. Within these limits, the results suggest that improving equity in physiotherapy care may benefit from approaches that go beyond non-discrimination and aim to foster safety, trust and comfort within the therapeutic relationship. Further research using larger and more diverse samples is needed to better understand these experiences.

REFERENCES: [1] Mohapatra A, Patwari S, Pansari M, Padhan S. Navigating Pain in Rheumatology: A Physiotherapy-Centric Review on Non-pharmacological Pain Management Strategies. Cureus 2023;15.
[2] Williams SL, Mann AK. Sexual and Gender Minority Health Disparities as a Social Issue: How Stigma and Intergroup Relations Can Explain and Reduce Health Disparities. Journal of Social Issues 2017;73:450–61.
Acknowledgments: NIL.
Disclosure of Interests: None declared.