fetching data ... 
Background: Patients with rheumatic and musculoskeletal diseases (RMDs) may be particularly vulnerable to weight stigma due to increased adiposity as a result of chronic pain, functional limitations, and disease-related changes in body weight. Despite its potential impact on psychological well-being and disease management, the prevalence of weight stigma in this population remains largely unexplored.
Objectives: To investigate the prevalence and correlates of internalized weight stigma in patients with different RMDs, and to examine whether demographic factors and type of RMD are associated with weight stigma scores.
Methods: This consecutive cross-sectional study included 44 outpatients from the Department of Rheumatology and Clinical Immunology at the University General Hospital of Larissa, interviewed between July 2024 and December 2024. Perceived weight stigma was assessed using the Perceived Weight Stigma Scale (PWSS) [1], with prevalence defined as the proportion of participants reporting at least one PWSS item >0. Internalized weight stigma was assessed using the Weight Self-Stigma Questionnaire (WSSQ) [2], including total score and subscales (Factor I: self-devaluation, Factor II: fear of enacted stigma). Reliability of PWSS and WSSQ scales was evaluated using Cronbach’s alpha. Group comparisons were conducted using non-parametric tests; Wilcoxon rank-sum tests compared stigma scores between sexes, and Kruskal-Wallis tests compared stigma scores across RMDs. Spearman’s rank correlation was used to assess associations between age, disease duration, and stigma scores. A multiple linear regression model was conducted to examine predictors of WSSQ. Age, sex, body mass index category, years since diagnosis, and primary diagnosis were first screened using univariate analyses, and predictors showing a trend or significant association were included in the multivariable model, using backward elimination. Statistical significance was set at p < 0.05, and all analyses were conducted using R (version 2025.09.2 + 418) [3].
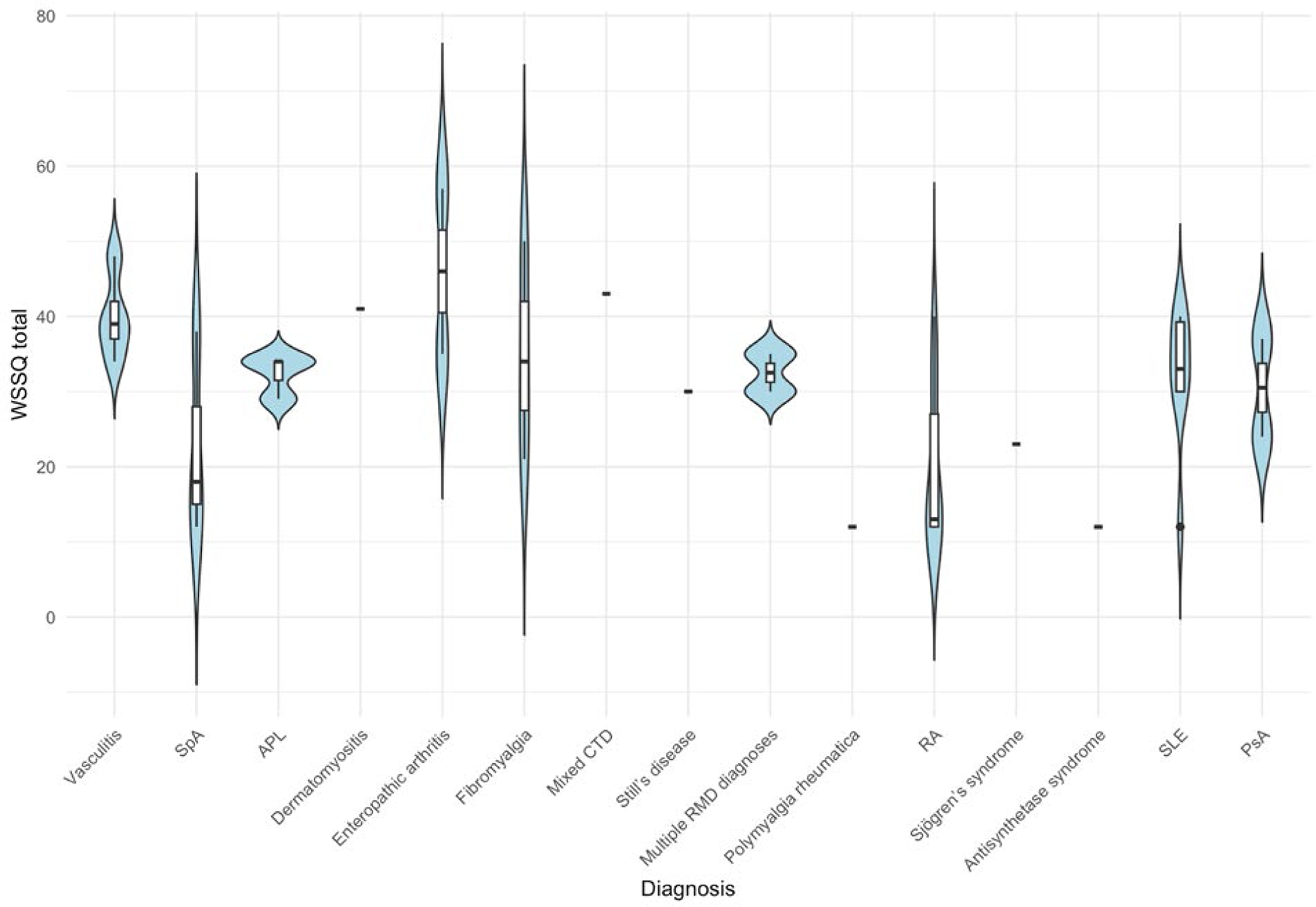
Results: The prevalence of PWSS was 27.1%, while WSSQ scores varied by diagnosis. Both the PWSS and WSSQ demonstrated good internal consistency, with Cronbach’s alpha of 0.90 and 0.91, respectively (WSSQ Factor I: α = 0.87, Factor II: α = 0.86). The mean WSSQ total score was 29.2 (median 31, IQR 17–38). In univariate analyses, older age showed a trend toward lower stigma (β = -0.25, p = 0.067), and longer disease duration was associated with lower stigma (β = -0.29, p = 0.044). In multivariable linear regression, age and primary diagnosis remained independent predictors of WSSQ total score (Adjusted R 2 = 0.33, p = 0.020). Compared with patients with vasculitis, those with a diagnosis of rheumatoid arthritis, polymyalgia rheumatica, spondyloarthritis, and antisynthetase syndrome demonstrated lower internalized stigma (Figure 3). No significant differences in the PWSS or WSSQ were observed between sexes (p = 0.368 and p = 0.577, respectively) or across primary diagnoses (Kruskal-Wallis p = 0.109 and p = 0.091, respectively).
Conclusions: Weight stigma is present among patients with RMD diagnoses, with internalized stigma varying by primary diagnosis. Interventions aimed at reducing stigma and supporting patients’ mental health should be considered alongside standard rheumatologic management.
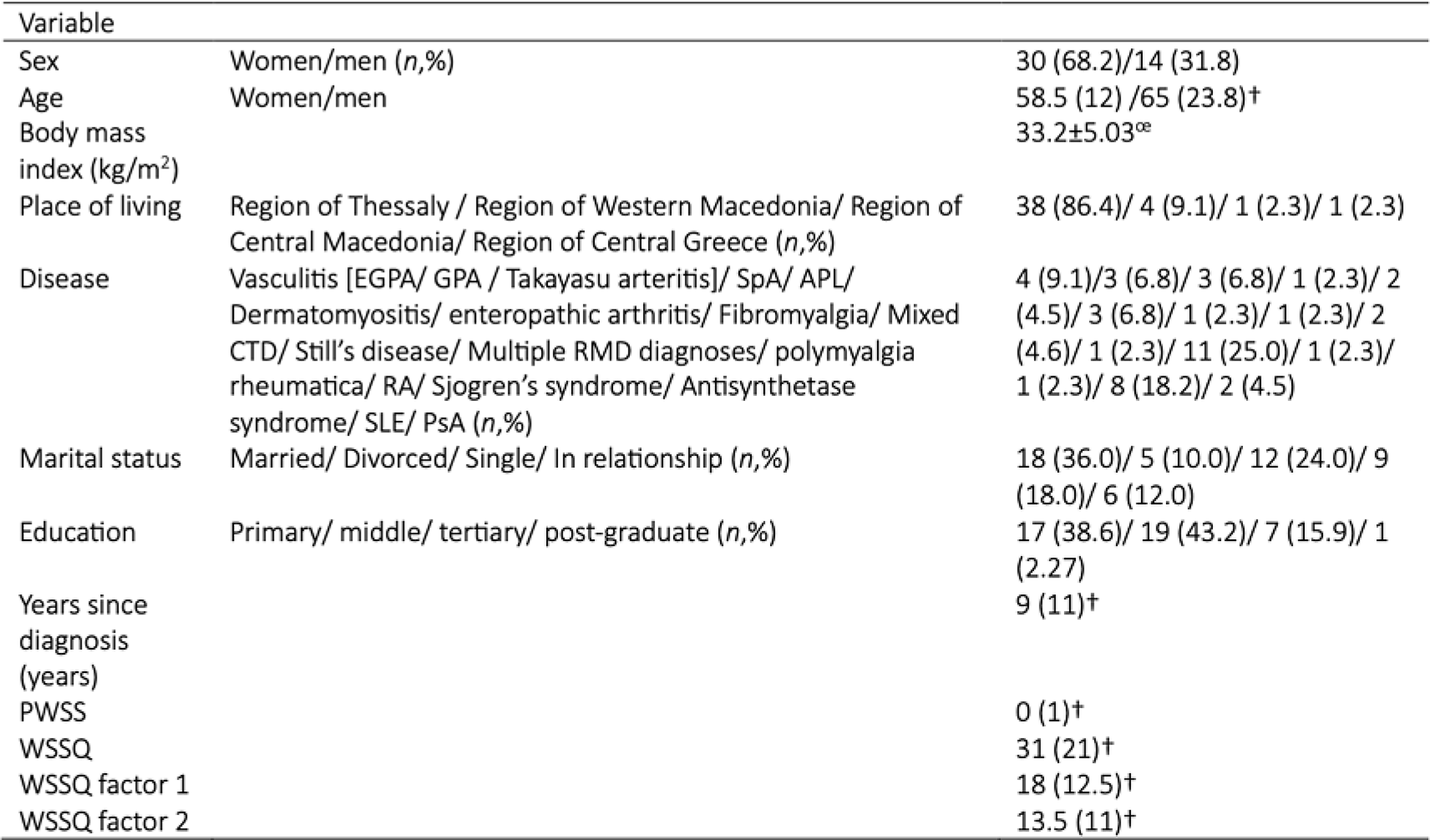
Characteristics of the patients (N=44).
APL: Antiphospholipid syndrome; EGPA: Eosinophilic Granulomatosis with Polyangiitis; GPA: Granulomatosis with polyangiitis; CTD: connective tissue disease; PsA: Psoriatic arthritis; PWSS: Perceived Weight Stigma Scale; RA: Rheumatoid arthritis; SLE: Systemic lupus erythematosus; SpA: Spondyloarthritis; WSSQ: Weight Self-Stigma Questionnaire; n : number of patients. œ mean ± SD; † median (IQR).
WSSQ among different rheumatic and musculoskeletal diseases (N=44).
APL: Antiphospholipid syndrome; CTD: connective tissue disease; RMD: rheumatic and musculoskeletal diseases; PsA: Psoriatic arthritis; RA: Rheumatoid arthritis; SLE: Systemic lupus erythematosus; SpA: Spondyloarthritis; WSSQ: Weight Self-Stigma Questionnaire.
REFERENCES: [1] Lin CY, Strong C, Latner JD, Lin YC, Tsai MC, Cheung P. Mediated effects of eating disturbances in the association of perceived weight stigma and emotional distress. Eat Weight Disord 2020;25:509–18.
[2] Lillis J, Luoma JB, Levin ME, Hayes SC. Measuring weight self-stigma: The weight self-stigma questionnaire. Obesity 2010;18:971–6.
[3] R Core Team. R: A Language and Environment for Statistical Computing. R Found Stat Comput Vienna, Austria 2016.
Acknowledgments: NIL.
Disclosure of Interests: None declared.