fetching data ... 
Background: Collaborating with patients as partners offers a means to enhance the inclusivity and real-world relevance of health research. This is particularly important in digital health given a growing policy drive towards digital transformation across healthcare systems[1,2]. While digital interventions offer exciting opportunities, they also risk widening inequities due to population disparities in digital literacy and access [3]. Digital health studies should therefore seek to embed a wide range of perspectives at every stage from design to delivery, as a foundation for the development of equitable interventions that serve diverse patient populations. The REmote MOnitoring of Rheumatoid Arthritis (REMORA) programme, running since 2015, has been profoundly shaped by its decade-long collaboration with a dedicated Patient and Public Involvement and Engagement (PPIE) group. Early work included co-designing a smartphone app for daily remote symptom tracking, and co-producing an educational video on patient self-assessment of tender and swollen joints[4,5]. The PPIE group continue to be instrumental in contributing to the entire REMORA2 programme, our ongoing 16-site stepped-wedge trial evaluating the clinical and cost-effectiveness of remote symptom tracking integrated into clinical systems and pathways [6].
Objectives: To report the processes and outputs of the REMORA programme’s PPIE collaborations with a focus on inclusivity.
Methods: Nine people living with rheumatoid arthritis (two males and seven females) were recruited from across the UK (Greater Manchester, London and Edinburgh) to join the REMORA2 PPIE group. Five have been involved since REMORA’s inception [7]. The group meet online quarterly, with minutes recorded and impact tracked using an established checklist [8]. Capacity building is supported with regular training opportunities. Reimbursement is appropriately budgeted following UK guidelines [9]. Governance is strengthened through the appointment of two patient co-leads, ensuring an effective patient steering role and shared accountability. The PPIE inclusivity agenda was informed by the findings of a feasibility study [10]. As REMORA2 progresses, additional activities are planned based on trial participant engagement patterns and feedback. Our PPIE approach aligns with EULAR recommendations for the involvement of patient research partners [11].
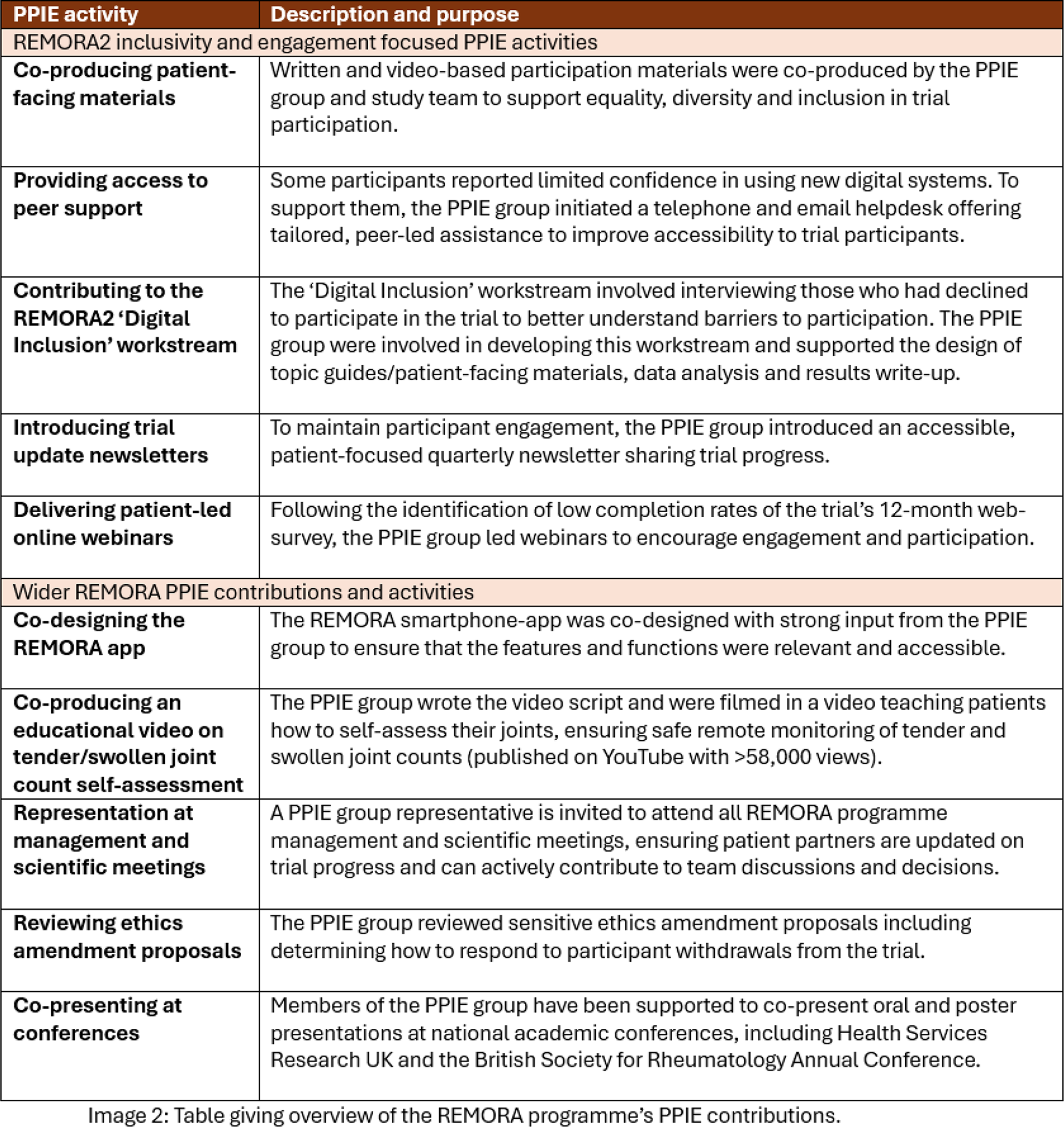
Results: To date, the REMORA2 PPIE group have directly initiated and led a number of inclusivity and engagement focused activities, including: co-producing patient-facing materials, providing access to peer support, contributing to a ‘Digital Inclusion’ workstream, introducing trial update newsletters and delivering patient-led online webinars. Figure 1 shows an example newsletter and trial instructional video.
The REMORA programme’s wider PPIE activities include: co-designing the REMORA smartphone app, co-producing an educational video on self-assessment of tender/swollen joints, representation at management and scientific meetings, reviewing sensitive ethics amendment proposals and co-presenting at conferences. Figure 2 provides further details on REMORA’s PPIE contributions.
Conclusions: Authentic patient partnership in digital health research can enhance the inclusivity and patient-centredness of both the technologies developed and the trials evaluating them. As digital interventions such as remote monitoring are increasingly explored to address healthcare challenges in rheumatology and beyond, it is critical that health inequities are not inadvertently widened. In this context, the REMORA programme has championed meaningful collaboration between researchers and patient partners, resulting in an inclusive digital health study that has been responsive to participants’ needs. By seeking regular and meaningful patient partner feedback, incorporating this into the programme, and tracking impact, we have gained valuable insights into inclusive PPIE practice in digital health research, which can inform future digital health studies.
REFERENCE: [1] de Thurah A et al (2022) EULAR points to consider for remote care in rheumatic and musculoskeletal diseases. Ann Rheum Dis. doi:10.1136/annrheumdis-2022-222341 [2]
GOV.UK. 10 Year Health Plan for England: fit for the future. 2025.
[3] Badr J et al (2024) Digital health technologies and inequalities: A scoping review of potential impacts and policy recommendations. doi:10.1016/j.healthpol.2024.105122 [4]
Centre for Epidemiology Versus Arthritis. How to self-examine for tender and swollen joints in rheumatoid arthritis. 2021.
Sharp CA et al (2023) How to self-examine for tender and swollen joints: Co-producing a training video for people with rheumatoid arthritis, Rheumatol Adv Pract. doi:10.1093/rap/rkad015 [6]
van der Veer SN et al (2024) Remote monitoring of rheumatoid arthritis (REMORA): study protocol for a stepped wedge cluster randomized trial and process evaluation of an integrated symptom tracking intervention. Trials. doi:10.1186/s13063-024-08497-9 [7]
REMORA Project. Patient and public involvement and engagement (PPIE) group
Staniszewska S et al (2017) GRIPP2 reporting checklists: tools to improve reporting of patient and public involvement in research. Res Involv Engagem. doi:10.1186/s40900-017-0062-2. [9]
NIHR. Payment guidance for researchers and professionals involving people in research
Druce KL et al (2025) Preparing to deliver a stepped wedge cluster-randomised trial to test the effectiveness of daily symptom tracking integrated into electronic health records for managing rheumatoid arthritis: a mixed-methods feasibility trial. BMC Rheumatol. doi:10.1186/s41927-025-00464-4 [11]
de Wit et al (2024) EULAR recommendations for the involvement of patient research partners in rheumatology research: 2023 update. Ann Rheum Dis. doi:10.1136/ard-2024-225566.
Acknowledgments: NIL.
Disclosure of Interests: None declared.