fetching data ... 
Background: Rheumatoid arthritis (RA) is a systemic autoimmune disease characterised by chronic inflammation, progressive joint damage, and substantial disability [1]. Patients with active RA have venous thromboembolic events (VTE) incidence rates 50-100% higher than the general population [2]. High disease activity approximately doubles VTE risk in RA compared to remission states [3]. Janus kinase (JAK) inhibitors, including baricitinib, are effective RA oral therapies but have raised safety concerns related to VTE, major adverse cardiovascular events (MACE), malignancy, and serious infections [4]. Two FDA post approval safety trials, RA-BRIDGE (NCT03915964) and RA-BRANCH (NCT04086745), were conducted to generate comparative long term safety data for baricitinib versus TNFi in patients with RA enriched for VTE risk factors, who also had elevated cardiovascular, malignancy and infection risk due to their older age and/or obesity.
Objectives: To evaluate the long-term safety of baricitinib compared with TNFi in patients with RA at increased risk of VTE in two post-marketing studies.
Methods: RA-BRIDGE (global) and RA-BRANCH (US based) are randomized, open label, active controlled safety trials. Adults with moderate to severe RA and ≥1 predefined VTE risk factor; prior VTE, age ≥60 years, body mass index (BMI) ≥30 kg/m 2 , or age 50 - <60 with BMI 25 - <30 k kg/m 2 , were randomized 1:1:1 to baricitinib 2 mg qd, baricitinib 4 mg qd, or TNFi (adalimumab or etanercept; administered according to local product label). Analyses were conducted on the safety population (randomized patients who received ≥1 dose of study drug). The primary analysis was based on on-treatment exposure with censoring at treatment discontinuation. Data from both studies were pooled according to the prespecified analysis plan. The primary endpoint was time from first dose to first VTE event; noninferiority of baricitinib (combined doses) versus TNFi was assessed using a prespecified margin of 1.8 for the upper limit of the 95% CI of the hazard ratio. Secondary endpoints included MACE, arterial thromboembolic events (ATE), malignancy (excluding nonmelanoma skin cancer (NMSC)), serious infections (SI) and opportunistic infections. Secondary endpoints were non-confirmatory without multiplicity adjustment. VTE, MACE, ATE, and opportunistic infections were confirmed by independent blinded adjudication committees. Incidence rates (IRs) and Hazard ratios (HRs) with 95% CIs were estimated for VTE and other safety outcomes using Cox proportional hazards models stratified by study and randomisation factors.
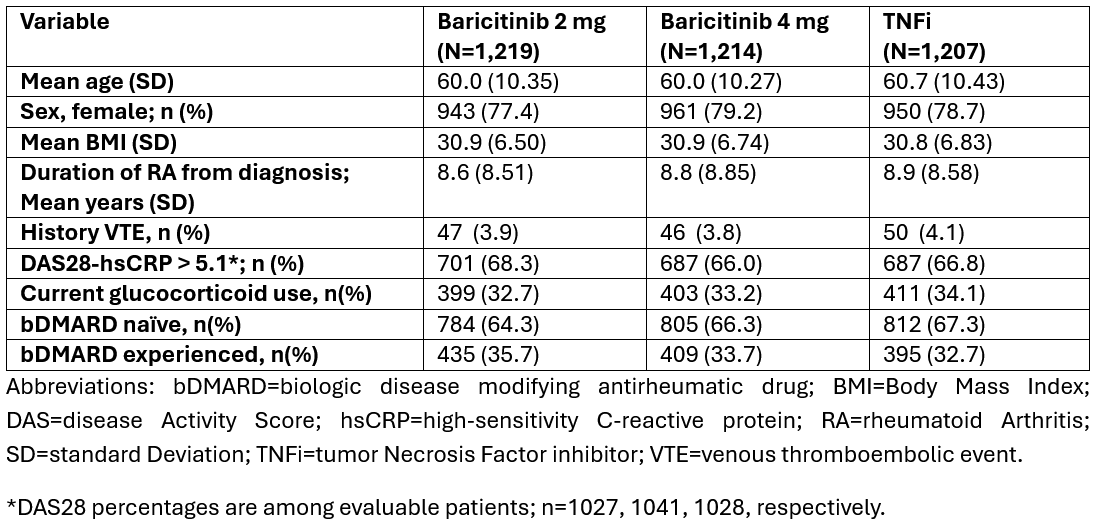
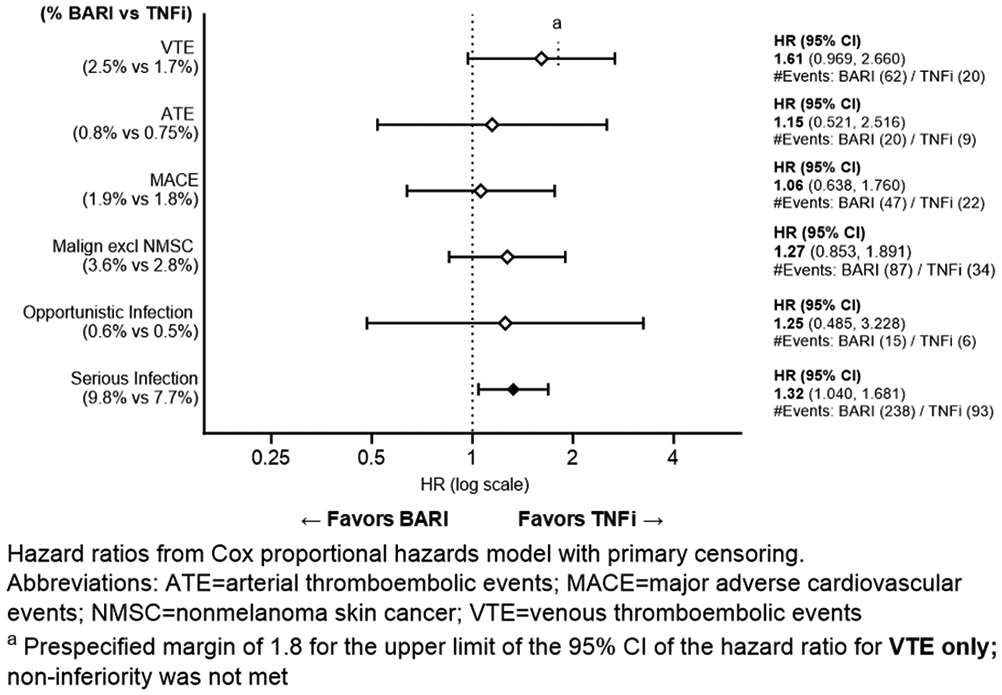
Results: A total of 3,640 patients were included in the combined RA-BRIDGE and RA-BRANCH population (baricitinib 2 mg, n=1,219; baricitinib 4 mg, n=1,214; TNFi, n=1,207) contributing to a total of 7694.4 patient years of exposure (PYE) for baricitinib and 3830.1 PYE for TNFi. Median on-treatment exposure was ~3.7 years in both groups. IRs were calculated per 100 PY using event-specific person-time. Patient baseline characteristics are shown in Table 1. Treatment discontinuation rates were balanced across arms (Baricitinib 55.2%; TNFi 57.3%) with similar rates due to adverse events (~14%) and patient withdrawal (14%). The HR for time to first adjudicated VTE for combined baricitinib versus TNFi was 1.61 (95% CI 0.97–2.66; p=0.066); baricitinib IR 0.79 (95% CI 0.60-1.01; 62 events); and TNFi IR 0.51 (95% CI 0.31-0.79; 20 events). The upper limit of the 95% CI exceeded the prespecified margin of 1.8; noninferiority was not demonstrated. Results were consistent across baricitinib doses (2mg HR 1.70; 95% CI 0.94-3.08; 4mg HR 1.69; 95% CI 0.97-2.94) with no dose dependent effect observed. The hazard ratios and 95% CIs across endpoints for baricitinib vs TNFi are shown in Figure 1. The risk of MACE was similar between combined baricitinib versus TNFi groups (HR 1.06; 95% CI 0.64–1.76). The risk of malignancy excluding NMSC was similar between baricitinib and TNFi (HR 1.27; 95% CI 0.85–1.89) with numerically higher rates in the 2-mg baricitinib group (IR 1.28; 95% CI 0.90-1.75) versus the 4-mg group (IR 0.94; 95% CI 0.67-1.29) and the TNFi group (IR 0.83; 95% CI 0.57-1.15). Serious infections were more frequent with baricitinib than TNFi (IR 3.17 vs. 2.46; HR 1.32; 95% CI 1.04–1.68). Covid-19 accounted for ~20% and ~13% of SI events in the combined baricitinib and TNFi groups, respectively. ATE, opportunistic infections and mortality were similar between groups.
Conclusions: In active RA patients enriched for VTE risk factors with high baseline disease activity (Table 1), noninferiority of baricitinib versus TNFi for VTE was not shown. Baricitinib showed a numerically higher VTE rate vs TNFi though absolute rates were low for the enriched population studied in both groups. No increased MACE risk was observed (HR 1.06) while serious infections were increased in the baricitinib arm, including new onset Covid-19. The enriched population studied may limit direct extrapolation of these findings to the broader RA population, where baseline VTE and infection risk is lower. These results inform the ongoing benefit-risk characterization of baricitinib and support individualized treatment decisions accounting for patient-specific VTE and infection risk factors.
Table 1. Patient baseline characteristics; RA-BRIDGE, RA-BRANCH
Summary of Time to First Event Analysis, Safety Population, Cox PH Model: Primary Censoring, Primary Analysis Model
REFERENCES:
[1] Sanchez-Florez JC, Seija-Butnaru D, Valero EG et al., J Pain Palliat Care Pharmacother. 2021;35(4):291-9.
[2] Molander V, Bower H, Frisell T,et al., Ann Rheum Dis. 2023;82(2):189-97.
[3] Molander V, Bower H, Frisell T et al. Ann Rheum Dis. 2021 Feb;80(2):169-175.
[4] Mori S, Ogata F, Tsunoda R. Clin Rheumatol. 2021 Nov;40(11):4457-4471.
Acknowledgments: NIL.
Disclosure of interest: Peter C. Taylor AlfaSigma, AbbVie, Gilead Sciences, Inc., Roche; Takeda; Eli Lilly; Nordic Pharma; and UCB; Immunovant; Moonlake; Sanofi, Alfasigma, Jeffrey Curtis Amgen, Abbvie, Janssen, Pfizer, Lilly, Amgen, Abbvie, Janssen, Pfizer, Lilly, Jon T. Giles Pfizer Inc., AbbVie, Eli Lilly, Novartis, Sana, Merck, Roy Fleischmann AbbVie, Almirall, Anaptys, Artiva Biotherapeutics, Atomwise, Biohaven Pharmaceuticals, BMS. Cyoxone, Deep Cure, Dren Bio, ECOR, Eisai, Galvani, Gates Bio, Genentech, Gilead, GSK, Halia, Immunovant, ImmuneMed, InventisBio, Istesso, Janssen, Janux, Eli Lilly, MSD, Monte Rosa, Overland, Novartis, Pfizer, Roche, RPharm, Synact, TPG, UCB, Vyne, and Xencor, Grace Wright AbbVie, AstraZeneca, Bristol Myers Squibb, Eli Lilly, Johnson & Johnson, Novartis, Sanofi, UCB., AbbVie, Amgen, AstraZeneca, Bristol Myers Squibb, Eli Lilly, Fate Therapeutics, Johnson & Johnson, Novartis, Pfizer, Sanofi, Scipher Medicine, SOBI, UCB., Elizabeth Perkins Eli Lilly and Company, AbbVie, BMS, Johnson & Johnson, Lilly, Novartis, UCB, Deepak L. Bhatt SandboxAQ, Tourmaline Bio, Viatris; Board of Directors: American Heart Association New York City, Angiowave, Bristol Myers Squibb (stock), DRS.LINQ, High Enroll, Alnylam, Altimmune, Broadview Ventures, Corcept Therapeutics, Corsera, GlaxoSmithKline, Hims, Sanofi, SERB, SFJ, Summa Therapeutics, Worldwide Clinical Trials; Acesion Pharma, Assistance Publique-Hôpitaux de Paris, Baim Institute for Clinical Research, Boston Scientific (Chair, PEITHO trial), Cleveland Clinic, Contego Medical (Chair, PERFORMANCE 2), Duke Clinical Research Institute, Mayo Clinic, Mount Sinai School of Medicine (for the ABILITY-DM trial, funded by Concept Medical; for ALLAY-HF, funded by Alleviant Medical), Novartis, Population Health Research Institute; Rutgers University (for the NIH-funded MINT Trial); American College of Cardiology (Senior Associate Editor, Clinical Trials and News, ACC.org; Chair, ACC Accreditation Oversight Committee), Arnold and Porter law firm (work related to Sanofi/Bristol-Myers Squibb clopidogrel litigation), Baim Institute for Clinical Research (AEGIS-II executive committee funded by CSL Behring), Belvoir Publications (Editor in Chief, Harvard Heart Letter), Canadian Medical and Surgical Knowledge Translation Research Group (clinical trial steering committees), CSL Behring (AHA lecture), Duke Clinical Research Institute, Engage Health Media, HMP Global (Editor in Chief, Journal of Invasive Cardiology), Medtelligence/ReachMD (CME steering committees), MJH Life Sciences, Oakstone CME (Course Director, Comprehensive Review of Interventional Cardiology), Philips (Becker’s Webinar on AI), Population Health Research Institute, WebMD (CME steering committees), Wiley (steering committee). Angiowave, Antlia Bioscience, Bayer, Boehringer Ingelheim, CellProthera, Cereno Scientific, E-Star Biotech, High Enroll, Janssen, Level Ex, McKinsey, Medscape Cardiology, Merck, NirvaMed, Novo Nordisk, Repair Biotechnologies, Stasys, SandboxAQ (stock options), Tourmaline Bio, Viatris; Board of Directors: American Heart Association New York City, Angiowave (stock options), Bristol Myers Squibb (stock), DRS.LINQ (stock options), High Enroll (stock);, Abbott, Acesion Pharma, Afimmune, Alnylam, Amarin, Amgen, AstraZeneca, Atricure, Bayer, Boehringer Ingelheim, Boston Scientific, CellProthera, Cereno Scientific, Chiesi, Cleerly, CSL Behring, Faraday Pharmaceuticals, Fractyl, Idorsia, Janssen, Javelin, Lexicon, Lilly, Medtronic, Merck, MiRUS, Moderna, Novartis, Novo Nordisk, Pfizer, PhaseBio, Regeneron, Reid Hoffman Foundation, Roche, Sanofi, Stasys, 89Bio, Torsten Witte AbbVie, Alfasigma, Boehringer Ingelheim, Celltrion, Chugai, Janssen, Lilly, Novartis, Pfizer, UCB, AbbVie, Alfasigma, Amgen, AstraZeneca, Boehringer Ingelheim, CSL Behring, GlaxoSmithKline, Janssen, Lilly, Medac, Nordic, Novartis, Sanofi, Takeda, UCB, Viatris, Masayoshi Harigai AbbVie, Asahi Kasei Pharma, AstraZeneca, Ayumi Pharmaceutical, Boehringer Ingelheim, Bristol Myers Squibb, Chugai Pharmaceutical, Eisai, Eli Lilly, Gilead Sciences, Kissei Pharmaceutical, Mitsubishi Tanabe Pharma, Mochida Pharmaceutical, Ono Pharmaceutical, Pfizer, Taisho Pharmaceutical, AbbVie, Boehringer Ingelheim, Bristol Myers Squibb, Kissei Pharmaceutical, AbbVie, Asahi Kasei Pharma, Ayumi Pharmaceutical, Boehringer Ingelheim, Chugai Pharmaceutical, Eisai, Eli Lilly, Kaken Pharmaceutical, Mitsubishi Tanabe Pharma, Mochida Pharmaceutical, Nippon Kayaku, Nippon Shinyaku, Pfizer, Taisho Pharmaceutical, Viatris, Rieke Alten AbbVie, Alfasigma, BMS, Celltrion, Galapagos, Janssen, Eli Lilly and Company, Novartis, Pfizer, Roche, UCB, Viatris, AbbVie, Alfasigma, BMS, Celltrion, Galapagos, Janssen, Eli Lilly and Company, Novartis, Pfizer, Roche, UCB, Viatris, Walter Deberdt Eli Lilly and Company, Eli Lilly and Company, Conor O’Leary Eli Lilly and Company, Eli Lilly and Company, Rodica Rosu Eli Lilly and Company, Eli Lilly and Company, Louis Sanden Eli Lilly and Company, Eli Lilly and Company, Sandra Chinchilla Eli Lilly and Company, Eli Lilly and Company, Joseph O’Shea Eli Lilly and Company, Eli Lilly and Company, Burcu Vardar Eli Lilly and Company, Eli Lilly and Company, Natasha Troy Eli Lilly and Company, Eli Lilly and Company, Jens Gerwien Eli Lilly and Company, Eli Lilly and Company, Josef S. Smolen AbbVie, Ananda, Astro, BMS, Celltrion, Chugai, Eli Lilly and Company, Immunovant, Janssen, MSD, Novartis, Pfizer, Roche, R-Pharma, Samsung, Sanofi, UCB, AbbVie, Astra-Zeneca, Eli Lilly and Company, Galapagos, Novartis