fetching data ... 
Background: Sjögren’s disease (SjD) is a systemic autoimmune disease primarily affecting the salivary and lacrimal glands. The clinical presentation is heterogeneous and can manifest as systemic organ involvement and symptoms of dryness, fatigue and pain [1]. Although the pathogenesis of SjD has not been fully elucidated, type-I interferon (IFN) signaling is considered as one of the key immune pathways involved [2,3]. Anifrolumab is a fully human, IgG1κ monoclonal antibody to the type-I interferon receptor subunit 1 and blocks the action of type-I IFNs. In patients with systemic lupus erythematosus (SLE), a systemic autoimmune disease that is pathogenetically linked to SjD and also marked by type-I IFN activity, anifrolumab has shown clinical efficacy based on a composite endpoint in a large phase-III trial [4]. We hypothesized that inhibition of type-I IFN signaling by anifrolumab may reduce systemic and glandular inflammation and attenuate disease activity in patients with SjD.
Objectives: To assess the clinical efficacy and safety of anifrolumab in patients with SjD, and study its mechanism of action.
Methods: This study was a randomized, double-blind, placebo-controlled phase IIa exploratory proof-of-mechanism trial. Main inclusion criteria were: fulfilling 2016 ACR/EULAR classification criteria for SjD, disease duration of ≤10 years, presence of anti-SSA antibodies and presence of active systemic disease and/or an unacceptable patient symptom state (ESSDAI ≥5 and/or ESSPRI ≥5). At least 50% of patients needed to fulfil the ESSDAI ≥5 criterion. Thirty patients were randomized in a 2:1 ratio to either anifrolumab or placebo treatment. Allocation was stratified by low (<5) or moderate-to-high (≥5) ESSDAI score at screening. Participants received i.v. injections in a dosage of 300 mg or placebo every 4 weeks, for a treatment period of 24 weeks. The primary endpoint was Composite of Relevant Endpoints for Sjögren’s Syndrome (CRESS) response at week 24 [5]. The CRESS is a composite endpoint consisting of five items: systemic disease activity (ClinESSDAI), patient-reported symptoms (ESSPRI), tear gland (Schirmer/OSS), salivary gland (UWS/SGUS), and serology (IgG/RF). A CRESS responder is defined as response on ≥3 of 5 items. Secondary endpoints included safety, CRESS response at week 12, response at individual CRESS items, candidate Sjögren’s Tool for Assessing Response (STAR) response [6], minimal clinically important improvement (MCII) in ESSDAI (decrease of ≥3 points compared to baseline) and MCII in ESSPRI (decrease of ≥1 point or ≥15%). The main data-analysis was descriptive.
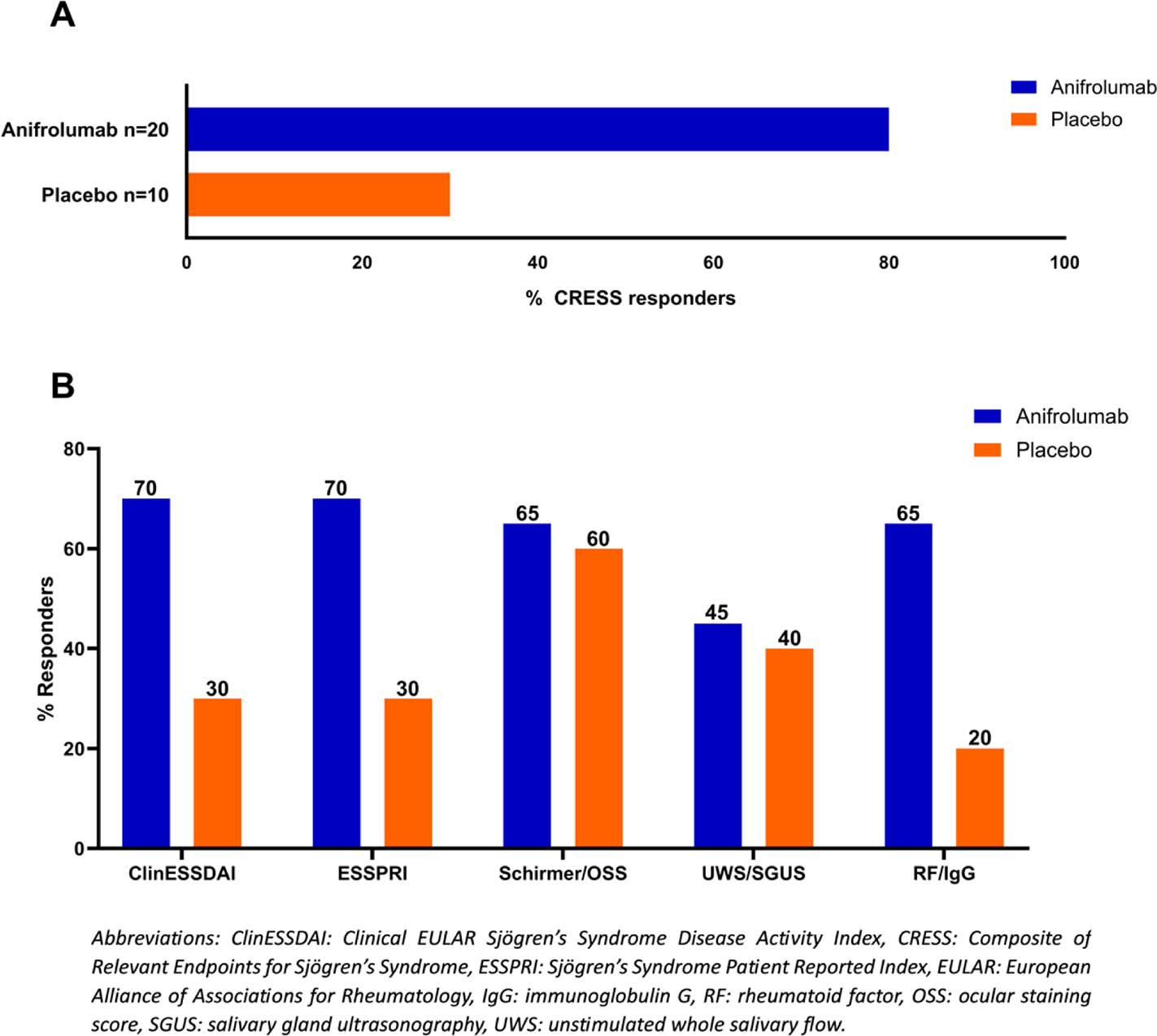
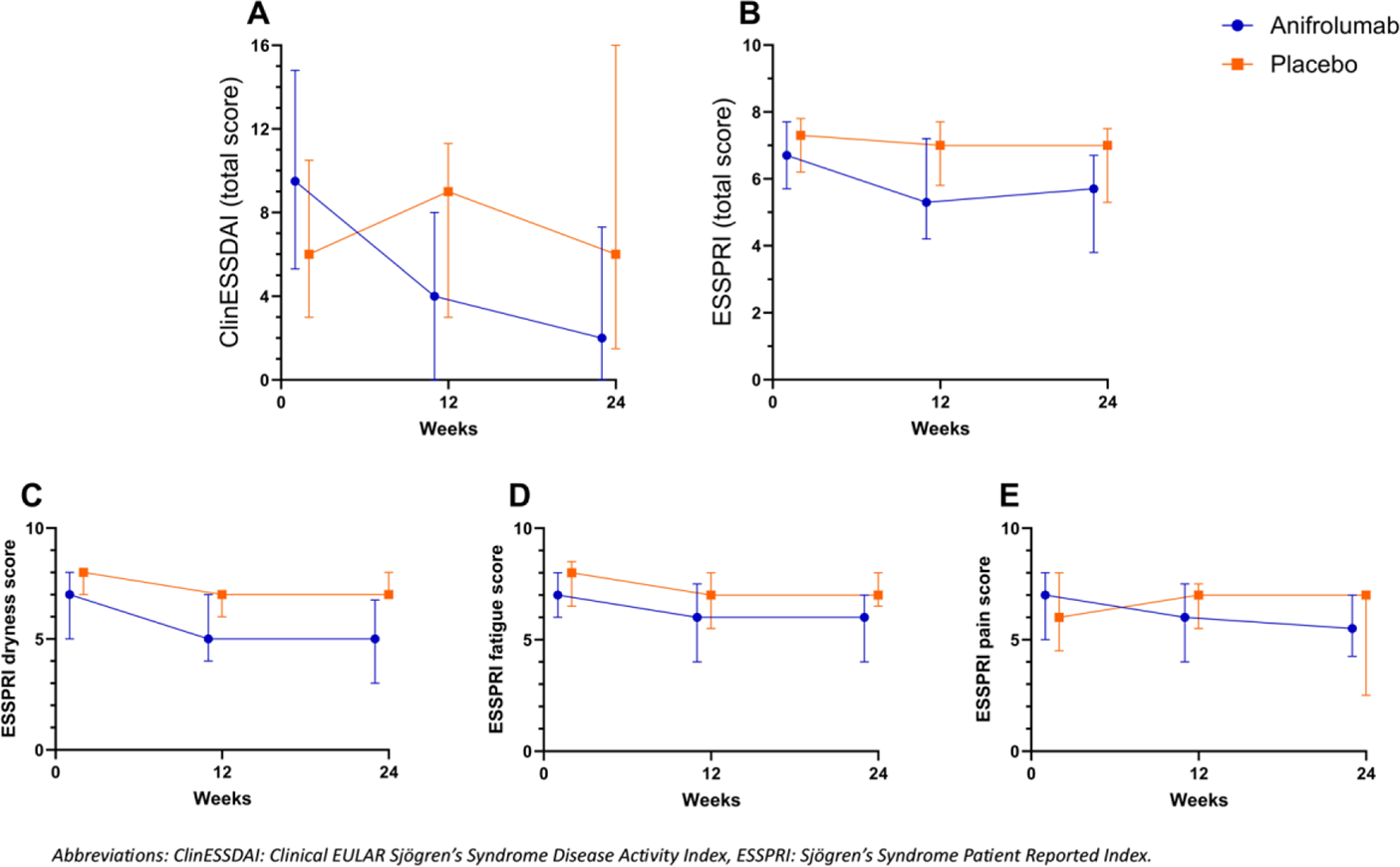
Results: Thirty participants were randomized, of whom 90% was female, 25 (83%) had ESSDAI ≥5 and 93% had ESSPRI ≥5. At baseline, the median (interquartile range [IQR]) age was 49 [31-58] years, disease duration 5 [2-9] years, median ESSDAI was 8 [6-12] and ESSPRI 6.7 [6.0-7.7]. All patients completed the study. At week 24, 16 (80%) patients were CRESS responder in the anifrolumab group compared to 3 (30%) patients in the placebo group (Figure 1A). Difference in response rate between treatment groups was also observed earlier in time. At week 12, 13 (65%) patients were CRESS responder in the anifrolumab group compared to 1 (10%) patient in the placebo group. Of the individual CRESS items, ClinESSDAI, ESSPRI and serological parameters showed the highest response rates in the anifrolimab group and the highest proportional differences between the anifrolumab and placebo groups (Figure 1B). Numerically larger improvements were found in ClinESSDAI total score, ESSPRI total score and all ESSPRI domain scores during treatment with anifrolumab compared to placebo (Figure 2). Furthermore, the anifrolumab group showed a higher proportion of participants who were candidate STAR responder (75% vs. 20%), reached MCII in ESSDAI (80% vs. 30%) and reached MCII in ESSPRI (70% vs. 30%) at week 24 compared to the placebo group. Additional secondary endpoints, including clinical, histological and immunological parameters are currently being analyzed. During the trial, there were no deaths or anaphylactic reactions and no cases of herpes zoster were observed. In total, 1 SAE (pneumonia) occurred in the anifrolumab group, which did not lead to treatment withdrawal. In general, anifrolumab was well tolerated. Infections were the most frequently observed AE, specifically nasopharyngitis, which was predominantly mild in intensity and resolved without needing treatment.
Conclusions: In this proof-of-mechanism trial with anifrolumab in SjD, we demonstrated numerically higher CRESS response in the anifrolumab group compared to placebo (80% vs. 30%, respectively). These findings support the rationale for therapeutic targeting of the type-I IFN pathway in SjD. Larger studies are needed to confirm efficacy and safety of anifrolimab in SjD.
CRESS response rates . A) Proportion of CRESS responders at week 24 in the anifrolumab group (n=20) and placebo group (n=10), B) Proportion of responders on the 5 individual CRESS items at week 24 in the anifrolumab and placebo groups.
ClinESSDAI and ESSPRI scores over time . (A) ClinESSDAI total score, (B) ESSPRI total score, (C) ESSPRI dryness score, (D) ESSPRI fatigue score, and (E) ESSPRI pain score (median with IQR) at baseline, week 12 and week 24 in the anifrolumab and placebo groups.
REFERENCES: [1] Brito-Zerón P, et al. Nature Reviews Disease Primers. 2016;2:16047.
[2] Bodewes ILA, et al. Rheumatology (United Kingdom). 2018;57(5):921–30.
[3] Soret P, et al. Nature Communications. 2021;12(1).
[4] Morand EF, et al. New England Journal of Medicine. 2020;382(3):211–21.
[5] Arends S, et al. Lancet Rheumatol 2021;3:e553–62.
[6] Seror R, et al. Ann Rheum Dis 2022;81:979–89.
Acknowledgments: NIL.
Disclosure of Interests: Hendrika Bootsma Argenx, AstraZeneca, Bristol-Myers Squibb, Novartis, Argenx, AstraZeneca, Bristol-Myers Squibb, Novartis, Noa S. Ausma: None declared, Liseth de Wolff: None declared, Greetje S. van Zuiden: None declared, Alja J. Stel: None declared, Lisette Olie: None declared, Konstantina Delli: None declared, Jamie Alberga: None declared, Fred K.L. Spijkervet: None declared, Frans G.M. Kroese Argenx, Novartis, Argenx, Bert van der Vegt MSD, Diaceutics, MSD and Visiopharm, AstraZeneca, Daiichi Sankyo, MSD, Philips, Visiopharm, Roche, IBEX, GE Healthcare, Philips, Owkin, Arjan Vissink: None declared, Gwenny M. Verstappen Bristol-Myers Squibb, Novartis, Argenx, Aurinia, Cullinan, AstraZeneca, Suzanne Arends Argenx, Bristol-Myers Squibb, Novartis.