fetching data ... 
Background: Self-management support is essential in managing rheumatoid arthritis (RA). Previously, the WebRA randomised controlled trial demonstrated that digital patient education improves self-efficacy, supports self-management, and reduces outpatient clinic visits [1]. Thus, digital patient education offers a promising alternative to traditional face-to-face approaches. The evidence on the cost-effectiveness of telehealth interventions in rheumatic and musculoskeletal diseases (RMDs) is mixed, showing both cost savings [2] and limited cost-effectiveness [3, 4]. To date, no studies have specifically evaluated the cost-effectiveness of digital patient education in RMDs.
Objectives: This trial aims to evaluate the 12-month cost-effectiveness of digital patient education compared to usual face-to-face patient education for patients with newly diagnosed RA from a societal perspective.
Methods: Adults newly diagnosed with RA were randomised to receive digital patient education or usual face-to-face patient education. Health related quality of life was measured using the EQ-5D-5L at baseline, and at 1, 3, 6, and 12 months. Utilities derived from EQ-5D-5L were used to estimate Quality Adjusted life-years (QALYs) as the primary effectiveness outcome. A secondary clinical effectiveness outcome was the proportion of patients achieving a minimal important change (MIC) in self-efficacy score from baseline to 12 months. Cost data were retrieved from national registries covering the 12-month intervention period and compared with a retrospective 12-month pre-intervention period. All direct and indirect costs from a societal perspective were included, comprising primary care services, prescription medications, hospital care, municipal services (preventive home visits, home care, rehabilitation, and nursing home), transport related to hospital contacts, and productivity loss due to sickness absence. Incremental cost-effectiveness ratios (ICERs) were estimated for both outcomes. A probabilistic sensitivity analysis was conducted, estimating the probability of cost-effectiveness at a willingness-to-pay threshold of €22,665 per QALY, based on the UK National Institute for Health and Care Excellence (NICE) reference threshold.
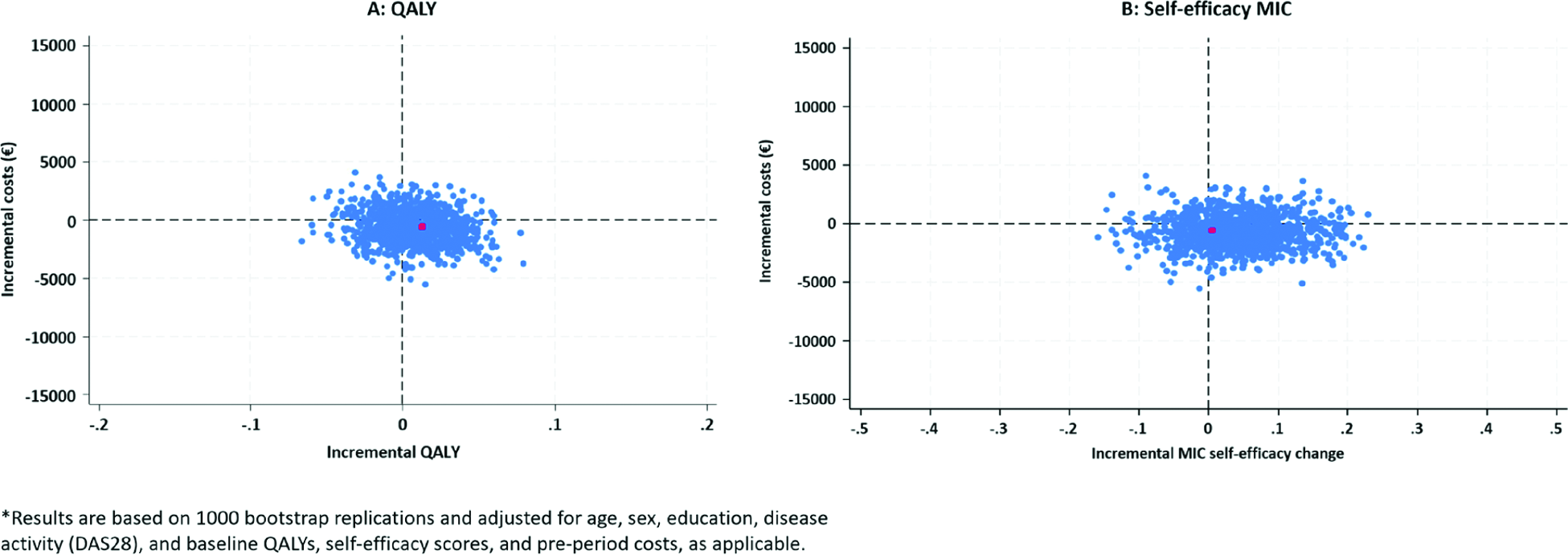
Results: Data from 175 of 180 participants were analysed (intervention: digital patient education, n=84; control: face-to-face patient education, n=91). The groups were well balanced in terms of age, gender, disease activity, and sociodemographic characteristics. In the intervention group, 60.7% were female, mean age was 58 years (SD 13.1), and mean disease activity score (DAS28) was 4.4 (SD 1.2). In the control group 61.5% were female, mean age was 56 years (SD 15.2), and mean DAS28 was 4.6 (SD 1.2). Digital patient education resulted in lower mean healthcare costs (€9,322 vs €9,886), and slightly greater QALY gains (mean difference 0.013). Hospital care constituted the largest cost component and the primary driver of cost differences between groups, with lower mean hospital costs in the digital patient education group (€5,485 vs 5,943). The intervention was dominant in both the adjusted (ICER: -€43,692/QALY) and the crude unadjusted model (ICER: -€24,056/QALY). In bootstrap analyses, 47.3% (adjusted) and 52.7% (unadjusted) of iterations fell in the south-east quadrant, indicating improved outcomes at lower costs (Figure 1A). The probability of cost-effectiveness was 70% at a willingness-to-pay threshold of €0/QALY and remained stable across increasing thresholds, reaching 71.5% at €22,665/QALY. For the secondary outcome (achieving MIC in self-efficacy), the intervention was cost-saving, but effects were small and inconsistent across adjusted and unadjusted analyses. In the adjusted analysis, 52.2% of bootstrap iterations were located in the south-east quadrant (lower costs, better outcomes), whereas in the unadjusted analysis, 52.2% fell in the south-west quadrant (lower costs, lower effectiveness) (Figure 1B).
Conclusions: Digital patient education demonstrates economic dominance over face-to-face patient education for QALY outcomes, with relatively high probability of cost-effectiveness across varying willingness-to-pay thresholds, supporting the hypothesis of resource savings for the healthcare system. While confirmation in broader populations is warranted, these findings suggest that structured digital patient education may be integrated into routine care to support efficient resource use without compromising quality.
ICER plots for the primary and secondary outcome*
REFERENCES: [1] Knudsen LR, et al. Rheumatology (Oxford). 2024;63(9):2547-56.
[2] Skovsgaard CV, et al. Scand J Rheumatol. 2023;52(2):118-28.
[3] Cuperus N, et al. Arthritis Care Res (Hoboken). 2016;68(4):502-10.
[4] Kloek CJJ, et al. BMC public health. 2018;18(1):1082.
Acknowledgments: NIL.
Disclosure of Interests: Line Raunsbæk Knudsen LEO Pharma, Amalie Wiben: None declared, Christian Skovsgaard: None declared, Mwidimi Ndosi: None declared, Ellen-Margrethe Hauge Novo, Novartis, AbbVie, SynACT Pharma, UCB., Novo Nordic Foundation, AlphaSigma, AbbVie, SynACT Pharma, Sobi, AbbVie, Novartis, Boehringer-Ingelheim., Kirsten Lomborg: None declared, Lene Wohlfahrt Dreyer: None declared, Lis Sørensen: None declared, Annette de Thurah: None declared