fetching data ... 
Background: Current therapies for rheumatoid arthritis (RA) primarily rely on sustained immunosuppression rather than immune tolerance restoration. As a consequence, durable immunosuppression-free remissions remain rare. Recent anecdotal reports have suggested that CD19-directed CAR T-cell therapy may be effective in RA [1-5]. However, controlled prospective data are lacking. Here, we present first prospective clinical and translational data evaluating CD19 CAR T-cell therapy in patients with treatment-refractory RA.
Objectives: To investigate the safety and efficacy of mivocabtagene autoleucel (miv-cel), an autologous, fully human CD19-directed CAR T-cell therapy, in patients with active, anti-citrullinated protein antibody (ACPA)-positive, treatment-refractory RA.
Methods: In phase I of the prospective, open-label phase I/II trial COMPARE (EU CT: 2024-514955-13-00), six adult patients with active, anti-citrullinated protein antibody (ACPA)-positive, treatment-refractory RA were enrolled. All patients received a single infusion of miv-cel, following fludarabine-cyclophosphamide lymphodepletion. All disease-modifying antirheumatic drugs were discontinued prior to CAR T-cell therapy. The primary endpoint was safety and tolerability within 4 weeks, assessed by the incidence and severity of cytokine release syndrome (CRS), immune effector cell-associated neurotoxicity syndrome (ICANS), and other adverse events. Key secondary endpoints included clinical disease activity, CAR T-cell expansion, duration of B-cell depletion, and changes in ACPA (anti-MCV) and rheumatoid factor (RF) titres. Patients were followed up for 16-36 weeks at the time of data cutoff.
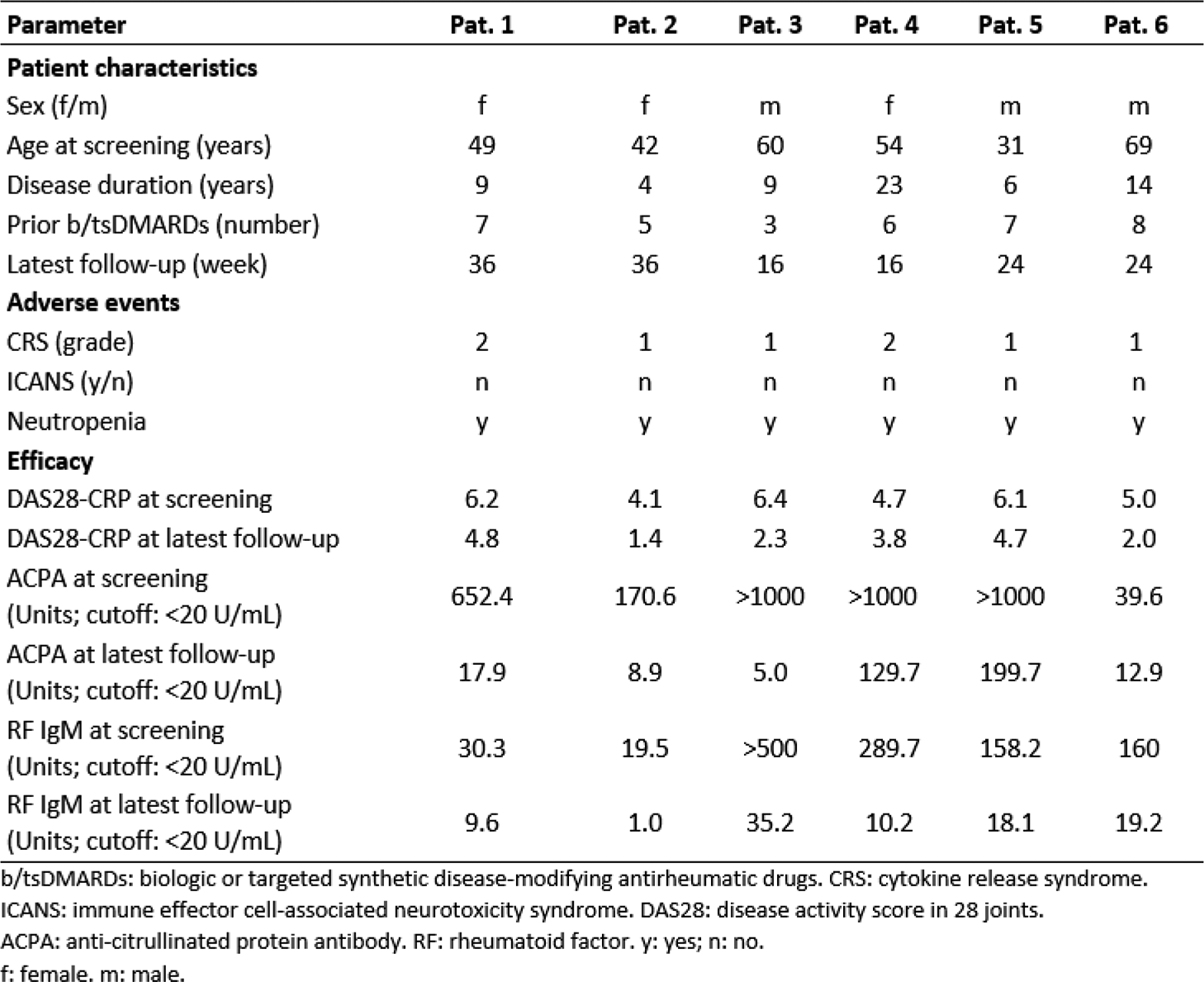
Results: Six patients (50% female) with a median age of 51.5 years (range 42-69) received treatment. Patients had high baseline disease activity (median DAS28-CRP 5.5, range 4.1–6.2) and extensive prior treatment exposure (median 6.5 b/tsDMARDs, range 3–8), including rituximab in four patients (Table 1). Patients were followed up for a median of 24 weeks (range 16-36). Miv-cel was generally well tolerated. CRS was limited to mild-to-moderate events (grade 1 in four patients; grade 2 in two patients). No ICANS and no unexpected toxicities occurred. All patients developed transient episodes of neutropenia (<1/nL). CAR T cells expanded rapidly, peaking at a median of 227.7 cells/µL (range 82.5–479.1) within three weeks after treatment, followed by a gradual decline. B cells were profoundly depleted in all patients, with reconstitution to normal levels (>0.1/nl) observed in two patients during follow-up. Autoantibody levels declined markedly, with sustained seroconversion to normal values (<20 U/mL) achieved in four patients for ACPA (66%) and in five patients for RF-IgM (83%). Disease activity decreased across all patients, with a median DAS28-CRP reduction of 41% (range 23-66) from screening to latest follow-up, and half of the patients achieved DAS28-CRP remission. With the exception of one patient who required glucocorticoid reintroduction because of a moderate flare after glucocorticoid withdrawal, all patients remained-off immunosuppressive therapy during follow-up.
Conclusions: In this first prospective evaluation of CD19 CAR T-cell therapy in ACPA-positive, treatment-refractory, active RA, miv-cel demonstrated a favourable safety profile and strong signals of clinical and serological efficacy. The depth of B-cell depletion, reduction of pathogenic autoantibodies, and early immunosuppression-free remission signals support the concept of an immunological reset in a significant proportion of patients.
Table 1. Patient characteristics, relevant adverse events and efficacy following CD19 CAR T-cell therapy
REFERENCES: [1] Haghikia A, et al. Ann Rheum Dis. 2024.
[2] Albach FN, et al. Rheumatology (Oxford). 2025.
[3] Lidar M, et al. Ann Rheum Dis. 2025.
[4] Li Y, et al. Cell res. 2025.
[5] Albach FN, et al. EULAR Rheumatology Open. 2025.
Acknowledgments: NIL.
Disclosure of Interests: Fredrik N. Albach: None declared, Marie Luise Hütter-Krönke: None declared, Marie Rehm: None declared, Murat Torgutalp: None declared, Thanh Hang Le: None declared, Ioanna Minopoulou: None declared, Artur Wilhelm: None declared, Arne Sattler: None declared, Johan Verhagen: None declared, Robert Biesen: None declared, Norman Michael Drzeniek: None declared, Edgar Wiebe: None declared, Anja Fleischmann: None declared, Vincent Casteleyn: None declared, Veronika Scholz: None declared, Thorben Witte: None declared, Tobias Alexander: None declared, Christian Furth: None declared, Jan Zernicke: None declared, Burkhard Muche: None declared, Sandra Hermann: None declared, Hans Ulrich Scherer: None declared, Rene Toes: None declared, Melanie Nuesch-Germano: None declared, Anne Pankow: None declared, Simon Schallenberg: None declared, Nadine Unterwalder: None declared, Alexander Pfeil: None declared, Elpida Phithak: None declared, Martin Krusche: None declared, Olaf Penack: None declared, Werner Stenzel: None declared, Manfred Wuhrer: None declared, Kamran Movassaghi: None declared, Eva Schrezenmeier: None declared, Thomas Vogl: None declared, Udo Schneider: None declared, Antonia Busse: None declared, Georg Schett: None declared, Ulrich Keller: None declared, Lars Bullinger: None declared, Arnd Kleyer Kyverna Therapeutics, Gerhard Krönke Kyverna Therapeutics, Kyverna Therapeutics, David Simon Kyverna Therapeutics, Kyverna Therapeutics.