fetching data ... 
Background: Structural damage, particularly new bone formation (NBF) and progression thereof in the spine, is a well-recognized feature of axial spondyloarthritis (axSpA). However, detecting structural damage progression in the spine has been challenging due to the low sensitivity to change of radiography, which is the conventionally used imaging technique.
In recent years, newer imaging modalities – including low-dose computed tomography (ldCT) and magnetic resonance imaging (MRI)-based synthetic CT (sCT) – have been investigated for their ability to detect structural spinal damage. sCT is a quantitative 3D MRI technique based on a multiple gradient-echo sequence and a deep-learning processing pipeline that can generate CT-like images without ionizing radiation. Previous studies have demonstrated that both ldCT and sCT have higher sensitivity and specificity in the detection of NBF compared to radiography, and that ldCT detects more structural progression than radiography over a two-year period [1, 2]. However, to our knowledge, no studies have evaluated the ability of ldCT to detect progression in the entire spine over time intervals shorter than two years, and no longitudinal studies of sCT of the spine have been conducted.
Objectives: To descriptively evaluate the capability of ldCT and sCT to detect the presence of NBF at baseline, and particularly the progression of NBF over one year in the spines of patients with axSpA.
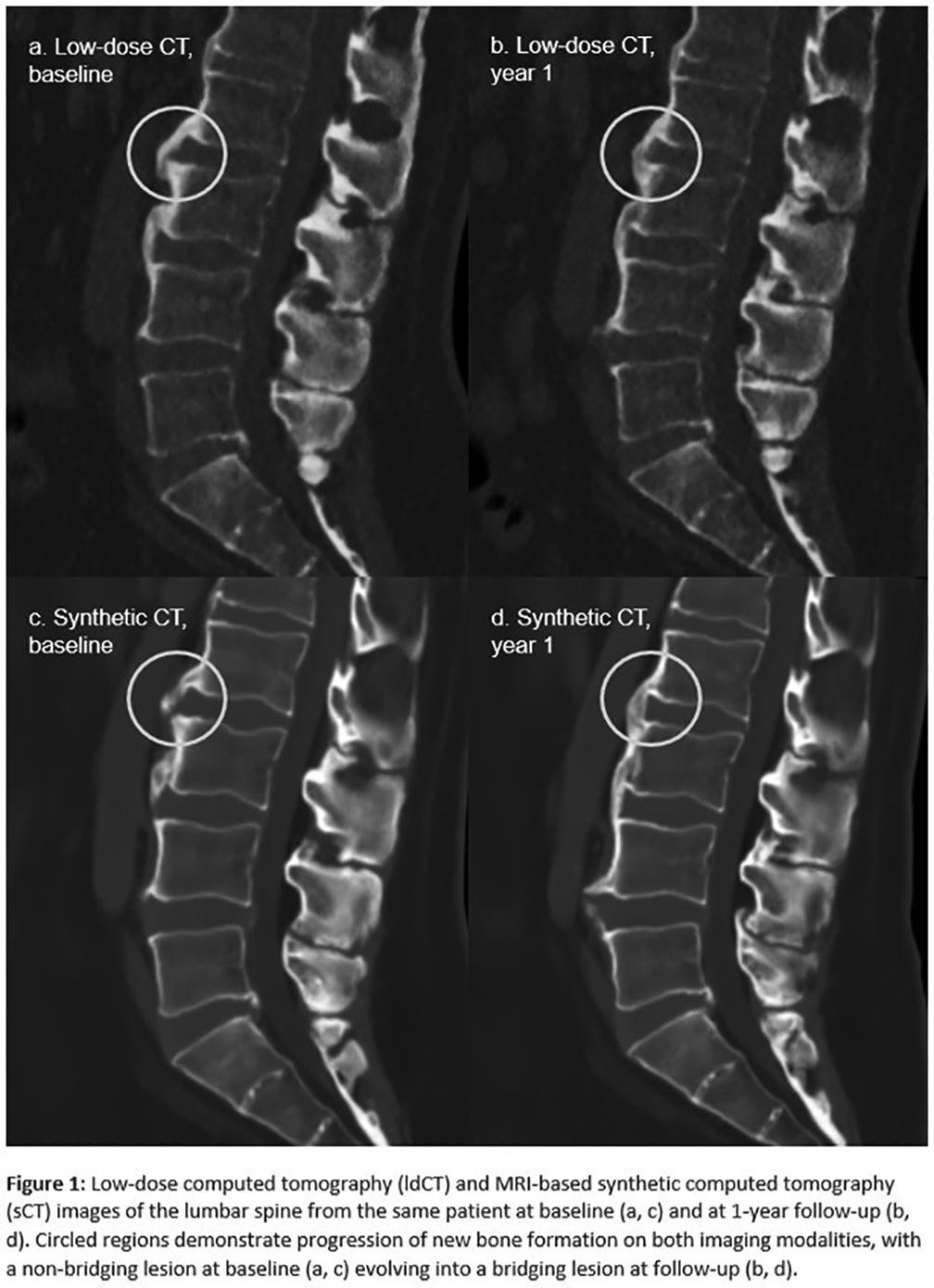
Methods: Patients meeting the Assessment of SpondyloArthritis international Society (ASAS) classification criteria for axSpA underwent clinical and laboratory assessments, as well as ldCT and MRI of the entire spine at baseline and after one year. sCT images were reconstructed from MRI using the BoneMRI application v.1.8. Both ldCT and sCT images were reconstructed in 3mm sagittal slice thickness. One reader evaluated ldCT and sCT images for the presence of NBF at each vertebral location (anterior corner, central segment, posterior corner) throughout the entire spine. The reader was unblinded to chronology but blinded to imaging modality and clinical information. Three types of NBF could be scored: 1) marginal syndesmophytes, 2) non-marginal syndesmophytes, and 3) osteophytes. Lesions were scored as 1 if present without bridging and 3 if bridging between vertebral units. Non-bridging lesions judged larger at one timepoint (compared to the other timepoint) could additionally be marked as “plus”. Descriptive statistics were performed, and change was calculated as the difference in scores between baseline and 1-year follow-up for both imaging modalities. In addition, the number of patients showing progression – defined as the development of a new lesion or growth of an existing lesion, including evolution from a non-bridging to a bridging lesion (Figure 1) or a lesion scored as “plus” at year 1 – and those showing regression, defined as the corresponding reverse changes, were calculated.
Sensitivity, specificity, and accuracy of sCT were determined using ldCT as the reference standard, and intraclass correlation coefficients (ICCs) were calculated to assess agreement between ldCT and sCT at both baseline and year 1.
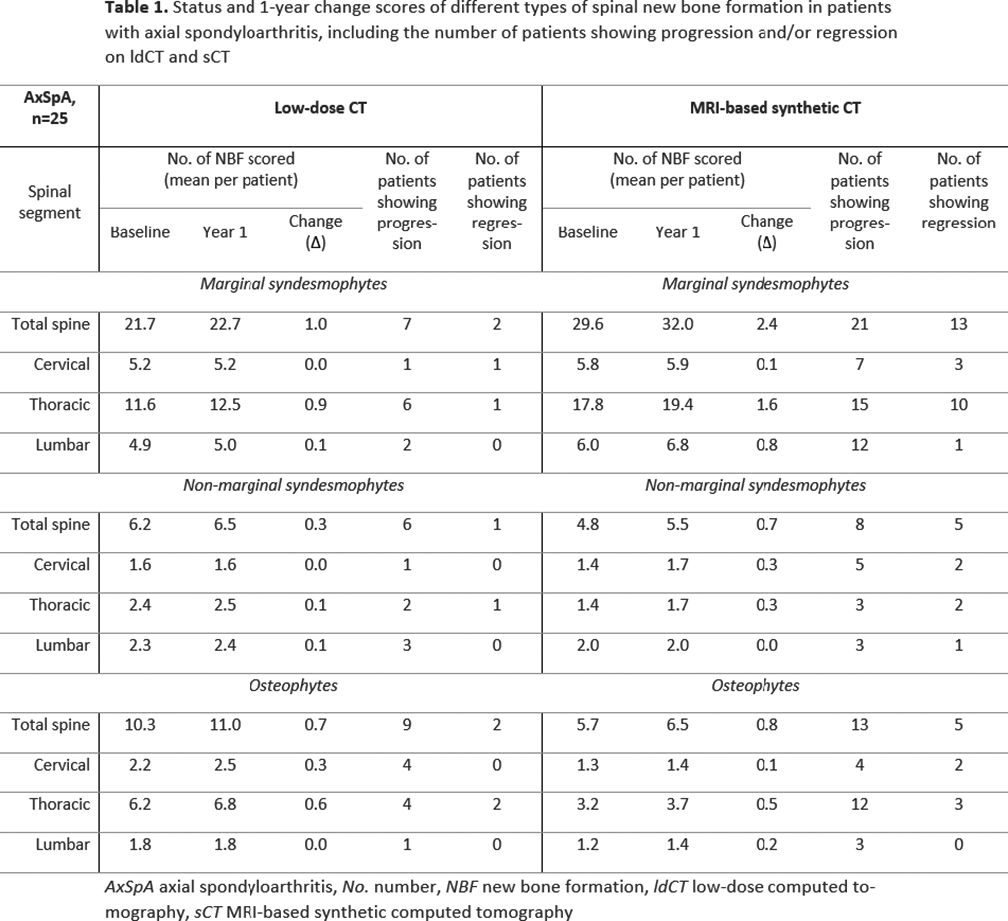
Results: 25 patients with axSpA were included (16 males, mean age 52.7 years). At baseline, a mean of 21.7 marginal syndesmophytes per patient was scored across the entire spine on ldCT, along with 6.2 non-marginal syndesmophytes and 10.3 osteophytes (Table 1). At year 1, mean ldCT scores per patient increased to 22.7 marginal syndesmophytes, 6.5 non-marginal syndesmophytes, and 11.0 osteophytes, corresponding to mean increases of 1.0, 0.3, and 0.7, respectively. On sCT, baseline whole-spine scores per patient were 29.6 for marginal syndesmophytes, 4.8 for non-marginal syndesmophytes, and 5.7 for osteophytes. At year 1, these increased to 32.0, 5.5, and 6.5, corresponding to mean per-patient increases of 2.4 marginal syndesmophytes, 0.7 non-marginal syndesmophytes, and 0.8 osteophytes.
The number of patients with progression of marginal syndesmophytes was 7 on ldCT and 21 on sCT, while regression was seen in 2 and 13 patients, respectively. For non-marginal syndesmophytes, progression was observed in 6 patients on ldCT and 8 on synthetic CT, and regression occurred in 1 patient on ldCT and 5 on sCT. For osteophytes, 9 patients showed progression on ldCT and 13 on sCT, whereas regression was observed in 2 patients on ldCT and 5 on sCT. Across all three types of lesions, most progression and regression occurred in the thoracic spine. Using low-dose CT as the reference standard, the sensitivity of synthetic CT for detecting marginal syndesmophytes was 0.81/0.81 at baseline/year 1; for non-marginal syndesmophytes, 0.54/0.54 at baseline/year 1; and for osteophytes, 0.41/0.42 at baseline/year 1. Specificity and accuracy were excellent (≥0.91) for all three lesion types at both timepoints.
ICCs between ldCT and sCT at baseline and year 1 were 0.90/0.87 for marginal syndesmophytes, 0.79/0.81 for non-marginal syndesmophytes, and 0.50/0.58 for osteophytes.
Conclusions: In this longitudinal study, 1-year progression of spinal NBF in patients with axSpA was observed on both sCT and ldCT. More patients showed progression on sCT than on ldCT; however, the overall magnitude of change for all lesions was comparable between modalities, warranting further investigation into methodological factors, including slice thickness selection. sCT showed good sensitivity and excellent specificity and accuracy at both baseline and follow-up compared with ldCT. With further refinement and validation, sCT and ldCT are promising options for longitudinal assessment of structural damage and progression in patients with axSpA, with sCT being favored by its radiation-free nature for use in both clinical trials and routine practice.
REFERENCES: [1] de Koning A, et al. Ann Rheum Dis. 2018;77:293-9.
[2] Willesen ST, et al. Ann Rheum Dis. 2024;83:807-15.
Acknowledgments: NIL.
Disclosure of Interests: Simone Tromborg Willesen: None declared, Jakob Møllenbach Møller: None declared, Kasper K Gosvig: None declared, Susanne Juhl Pedersen Novartis, UCB and AbbVie, Stylianos Georgiadis Novartis, UCB and AbbVie, Mikkel Østergaard Abbvie, BMS, Boehringer Ingelheim, Celgene, Eli Lilly, Galapagos, Gilead, Hospira, Janssen, MEDAC, Merck, Novartis, Novo, Orion, Pfizer, Regeneron, Roche, Sandoz, Sanofi, UCB, Abbvie, BMS, Boehringer Ingelheim, Celgene, Eli Lilly, Galapagos, Gilead, Hospira, Janssen, MEDAC, Merck, Novartis, Novo, Orion, Pfizer, Regeneron, Roche, Sandoz, Sanofi, UCB, AbbVie, Amgen, BMS, Merck, Celgene, Eli Lilly, Novartis, UCB.