fetching data ... 
Background: Growing evidence indicates that somatic mosaicism constitutes a mechanistic link between aging, chronic inflammation, and autoimmunity. Mosaic loss of the Y chromosome (mLOY) represents the most prevalent acquired somatic alteration in aging men. Giant cell arteritis (GCA) provides a unique model to investigate age related immune dysregulation in the setting of mLOY, as it exclusively affects individuals older than 50 years. The disease is closely related to polymyalgia rheumatica (PMR), and both conditions are increasingly regarded as manifestations of a shared GCA–PMR spectrum disease (GPSD).
Our research group has recently identified mLOY as a strong and independent predictor of relapse in GCA, associated with significantly reduced relapse free survival 1 . Moreover, a higher mLOY burden was linked to pronounced alterations in inflammatory signaling, particularly under tocilizumab therapy, including increased interleukin (IL)-6, IL-17, IL-23, interferon gamma, and tumor necrosis factor alpha signaling. While these findings position mLOY not merely as an epiphenomenon of aging but as a potential contributor to the initiation or persistence of pathogenic immune responses in GCA, its role within the broader GPSD remains unknown.
Objectives: To investigate mLOY across the GPSD and to evaluate its potential value as a phenotypic biomarker.
Methods: Patients with GCA and PMR were recruited at the Division of Rheumatology, University Hospital Bonn, Germany, between July 2024 and October 2025. Collected data included GCA related symptoms, disease manifestations, and laboratory parameters, including C-reactive protein and complete blood count. Comprehensive demographic, clinical, and treatment information was recorded. Multimodal imaging data, including vascular ultrasound, magnetic resonance imaging, and positron emission tomography-computed tomography, were obtained to assess vascular involvement. At inclusion, whole blood samples were collected. Genomic deoxyribonucleic acid (DNA) was isolated using the GeneJET Whole Blood DNA Purification Mini Kit, and DNA concentrations were normalized using a NanoDrop spectrophotometer (both Thermo Fisher Scientific). Burden of mLOY was quantified using a droplet digital polymerase chain reaction (PCR) system (Naica) with a 16,000 droplet chip and a single nucleotide polymorphism assay targeting a 6 bp difference between the AMELX and AMELY genes (Thermo Fisher Scientific). Data were analyzed with the manufacturer’s software, and the degree of LOY was calculated as 1 − (AMELY/AMELX concentration). Statistical analyses included a global comparison of mLOY fractions across clinical phenotypes and a predefined comparison between patients with isolated PMR and those with GCA. Exploratory analyses assessed associations between mLOY and clinical as well as immunoserological parameters. A p value < 0.05 was considered statistically significant.
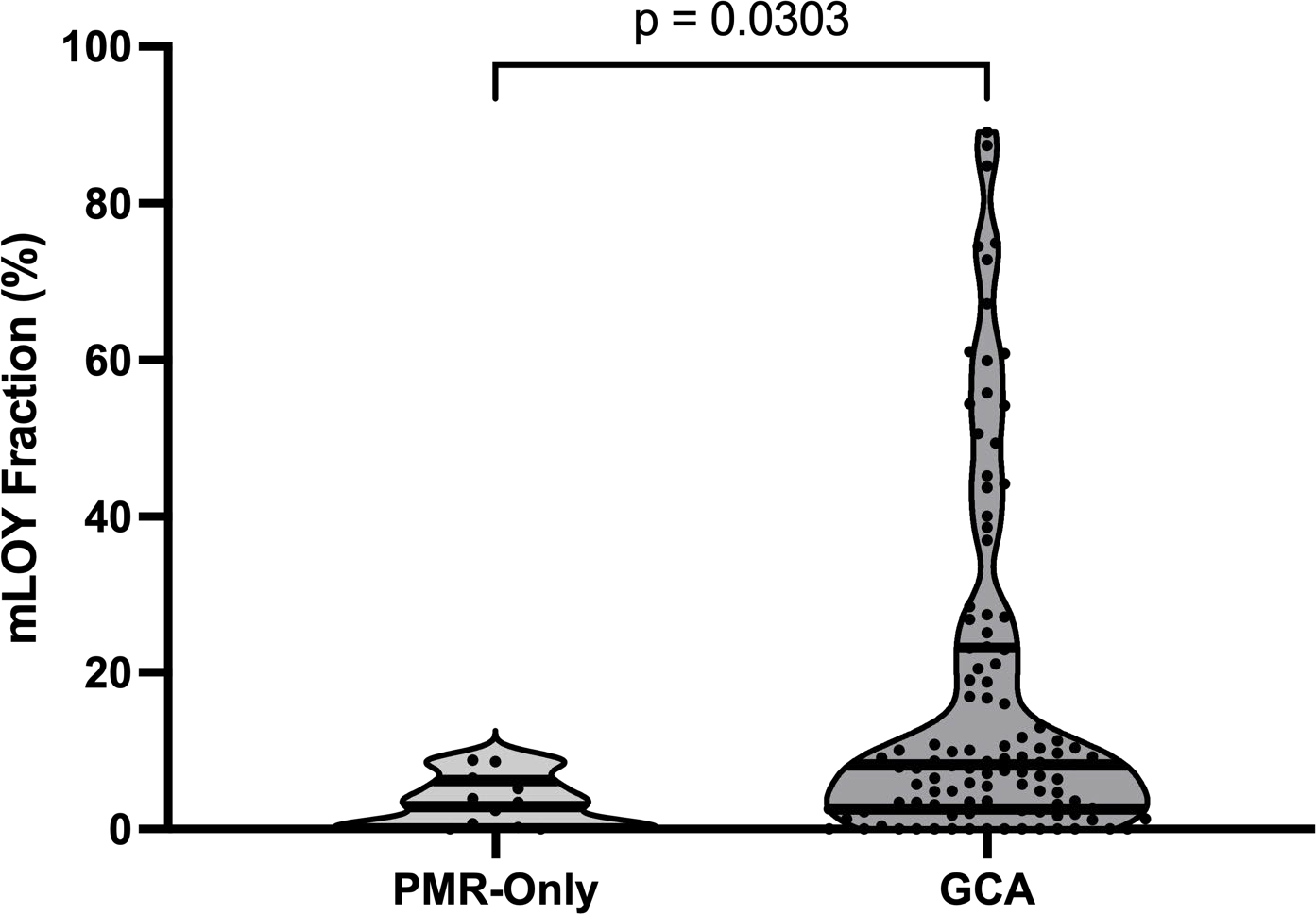
Results: A total of 88 patients with isolated GCA (mean age 74.0 ± 8.7 years), 12 patients with isolated PMR (73.5 ± 6.8 years), and 22 patients with combined GCA+PMR (72.6 ± 9.3 years) were included. The median mLOY fraction in the overall cohort was 16.2% (SD ± 21.9). Patients with isolated PMR exhibited a markedly lower mLOY burden (3.3%, SD ± 3.3) compared with patients with isolated GCA (17.5%, SD ± 22.9) and those with combined GCA+PMR (18.1%, SD ± 21.6). Overall, patients without GCA had significantly lower mLOY fractions than patients with GCA, irrespective of concomitant PMR (17.7%, SD ± 22.6; p = 0.030; Figure 1). No significant associations were observed between mLOY burden and GCA manifestation pattern (cranial versus large vessel involvement), systemic inflammatory markers at diagnosis or disease activity at time of inclusion (all p > 0.05).
Conclusions: This study is the first to demonstrate that mLOY burden differs significantly between GCA and isolated PMR phenotypes. Importantly, the association between mLOY and the GCA spectrum appears to be independent of systemic inflammatory activity and of phenotypic differentiation within GCA. Our findings suggest that mLOY may serve as a biomarker for immunophenotypic characterization across the GPSD and extend its role beyond prognostic factor toward phenotypic stratification within GPSD.
Burden of mLOY Across PMR-only and GCA Patients.
Figure 1 illustrates the distribution of mLOY within the GPSD: Patients with the presence of GCA exhibited higher mLOY percentages compared to those with PMR-only, with * = p<0.05 indicating statistical significance. Abbreviations: GCA = giant cell arteritis; GPSD = GCA – PMR spectrum disease; PMR = polymyalgia rheumatica; mLOY = mosaic loss of Y chromosome.
REFERENCES: [1] Petzinna SM, Kirch S-M, Adamson MS, et al. AYLo study-elevated relapse risk and dysregulated proinflammatory signalling in giant cell arteritis patients with mosaic loss of the Y chromosome. Ann Rheum Dis. 2025. doi:10.1016/j.ard.2025.06.2133.
Acknowledgments: NIL.
Disclosure of Interests: None declared.