fetching data ... 
Background: Recognising and understanding patients’ health literacy (HL) needs at the point of care is crucial to deliver effective, equitable and person-centered care. Nevertheless, healthcare providers (HCPs) in rheumatology find it challenging to intuitively recognise the diverse and (often) situational HL needs [1,2]. To support HCPs, the Conversational Health Literacy Assessment Tool for inflammatory Rheumatic Diseases (CHAT-iRD) was co-created with international rheumatology experts and patient research partners (PRPs), drawing on existing tools and clinical insights. Intended as a conversational guide, the CHAT-iRD provides specific prompts for questions and observations across four domains identified as most relevant: (1) ‘supportive relationships with HCPs’, (2) ‘supportive personal relationships’, (3) ‘health information access, comprehension and use’ and (4) ‘health behaviour and health promotion’.
Objectives: The aim of this study was to explore the acceptability and usability of the CHAT-iRD in clinical rheumatology practice, from the perspective of both HCPs and patients.
Methods: In this qualitative study, data were collected through individual semi-structured 1-hr interviews with rheumatology HCPs from The Netherlands, Germany and The United Kingdom (n=7) and through two 2-hr focus group interviews with patients with iRDs (one in-person in the Netherlands and one online with international PARE PRPs, total n=11). A facilitator presented the background and content of the CHAT-iRD, after which participants were asked to share their views regarding the acceptability and usability of the tool as a whole and the four domains separately. All interviews were transcribed verbatim, coded inductively via ATLAS.ti and analysed thematically, after which the emerging themes were structured into a conceptual model.
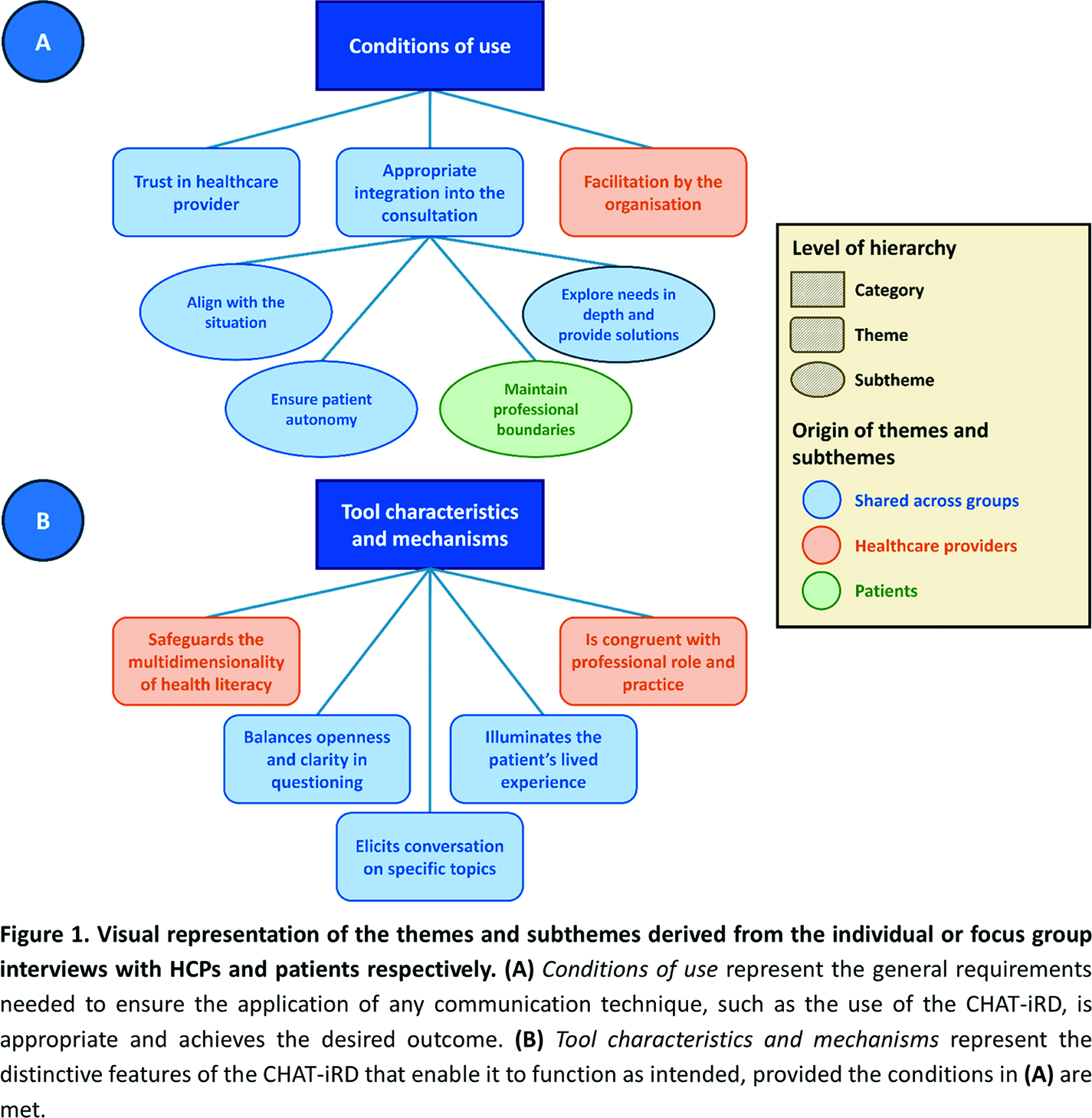
Results: Thematic analysis of the interview data revealed two overarching categories (Figure 1), covering a total of eight themes, one of which was subdivided into four subthemes. Most themes and subthemes were discussed by both HCPs and patients; three themes were specific to the HCP interviews, and one subtheme was specific to the patient focus groups. The first category, Conditions of use (Figure 1A), refers to the general requirements that need to be met to ensure a conversation guided by the CHAT-iRD is appropriate and achieves the desired outcome. These conditions are not unique to the CHAT-iRD but represent generic principles required for successful application of any communication technique. For instance, HCPs and patients mentioned that gaining meaningful insights from a dialogue requires a trusting relationship to ensure honest answers, should align with the specific situation and should explore needs in depth but also include solutions . The second category, Tool characteristics and mechanisms (Figure 1B), refers to the distinctive features of the CHAT-iRD that enable it to function as intended, provided that the aforementioned conditions are met. Broady speaking, these features characterise the tool as a guiding framework to cover the full scope of HL, while simultaneously acting as a catalyst for deepening the dialogue on relevant topics. For instance, rather than relying on intuition or focusing only on familiar aspects of HL, HCPs appreciated having a reference to discuss aspects of HL less familiar to them, to obtain the full picture (theme: ‘Safeguards the multidimensionality of health literacy’ ). Furthermore, where HCPs saw the CHAT-iRD as beneficial given it uncovers their blind spots about their patients’ lives, patients saw this as a sign of empathy and being heard (theme: ‘Illuminates the patient’s lived experience’ ).
Conclusions: The CHAT-iRD shows promise as a conversational aid for HCPs to assist the recognition of their patients’ diverse HL needs in rheumatology practice, offering a multidimensional lens to illuminate the patient’s reality and naturally elicit specific topics. Interestingly, the majority of themes were raised by both HCPs and patients. Both highlighted the required conditions for the tool’s use (Figure 1A) and pointed to relevant characteristics and mechanisms that make it work in practice (Figure 1B). Building on these findings, planned next steps involve the development of educational materials for HCPs, as well as determining the effectiveness of the updated CHAT-iRD and identifying facilitators and barriers for its use in rheumatology practice with a diverse patient population in three countries.
REFERENCES: [1] Bakker MM, Putrik P, Rademakers J, van de Laar M, Vonkeman H, Kok MR, Voorneveld-Nieuwenhuis H, Ramiro S, de Wit M, Buchbinder R, Batterham R, Osborne RH, Boonen A. Addressing health literacy needs in rheumatology: Which patient health literacy profiles need the attention of health professionals? Arthritis Care Res (Hoboken). 2021;73(1):100-9. doi: 10.1002/acr.24480.
[2] Bakker MM, Putrik P, Dikovec C, Rademakers J, Vonkeman HE, Kok MR, Voorneveld-Nieuwenhuis H, Ramiro S, de Wit M, Buchbinder R, Batterham R, Osborne RH, Boonen A. Exploring discordance between Health Literacy Questionnaire scores of people with RMDs and assessment by treating health professionals. Rheumatology (Oxford). 2023;62(1):52-64. doi: 10.1093/rheumatology/keac248.
Acknowledgments: NIL.
Disclosure of Interests: Jelle Pergens: None declared, Mark Matthijs Bakker Eli Lilly, Sandoz, Eli Lilly, Ioana Andreica UCB, GSK, Lilly, Alfasigma, Celltrion, UCB, GSK, Alfasigma, Celltrion, GSK, Mrinalini Dey: None declared, Olga Gershuni: None declared, Uta Kiltz AbbVie, Alfasigma, Eli Lilly, GSK, J&J, UCB, AbbVie, Alfasigma, Eli Lilly, GSK, J&J, UCB, AbbVie, Amgen, Fresenius, GBA, GSK, Hexal, Novartis, UCB, Souzi Makri: None declared, Elena Nikiphorou UCB, Pfizer, Gilead, Galapagos, AbbVie, Eli Lilly, Alfasigma, Fresenius, Novartis, UCB, Pfizer, Lilly, Annette de Thurah: None declared, Maarten de Wit: None declared, Annelies Boonen Johnson & Johnson, Abbvie, Phizer, UCB, AbbVie, Eli Lilly.