fetching data ... 
Background: Cardiovascular disease (CVD) is a leading cause of morbidity and mortality in juvenile-onset systemic lupus erythematosus (JSLE). There is an urgent unmet need for robust biomarkers capable of predicting atherosclerosis progression and therapeutic response, enabling personalised CVD risk stratification and management in young people with JSLE.
Objectives: To investigate whether novel serum autoantibody signatures can predict atherosclerosis progression and response to atorvastatin therapy in children and young people (CYP) with JSLE.
Methods: We conducted a biomarker discovery study using baseline serum samples from a sub-cohort of the APPLE (Atherosclerosis Prevention in Pediatric Lupus Erythematosus) trial [1], a large, multi-centre, randomised, double-blind clinical trial of atorvastatin versus placebo (1:1) conducted across 21 sites in North America, with carotid intima-media thickness (CIMT) progression over 36 months as the primary outcome. Ninety-four CYP with JSLE (45 randomised to placebo and 49 to atorvastatin) with matched baseline serum samples and CIMT data were included. Participants were stratified within each treatment arm according to CIMT progression patterns using unsupervised clustering. Functional serum proteomic analysis was performed on baseline serum samples (n=94) using the KREX platform. Empirical Bayes moderated t -tests and receiver operating characteristic (ROC) analysis with logistic regression were used to define serum autoantibody profiles predictive of high versus low atherosclerosis progression patterns in both APPLE trial arms.
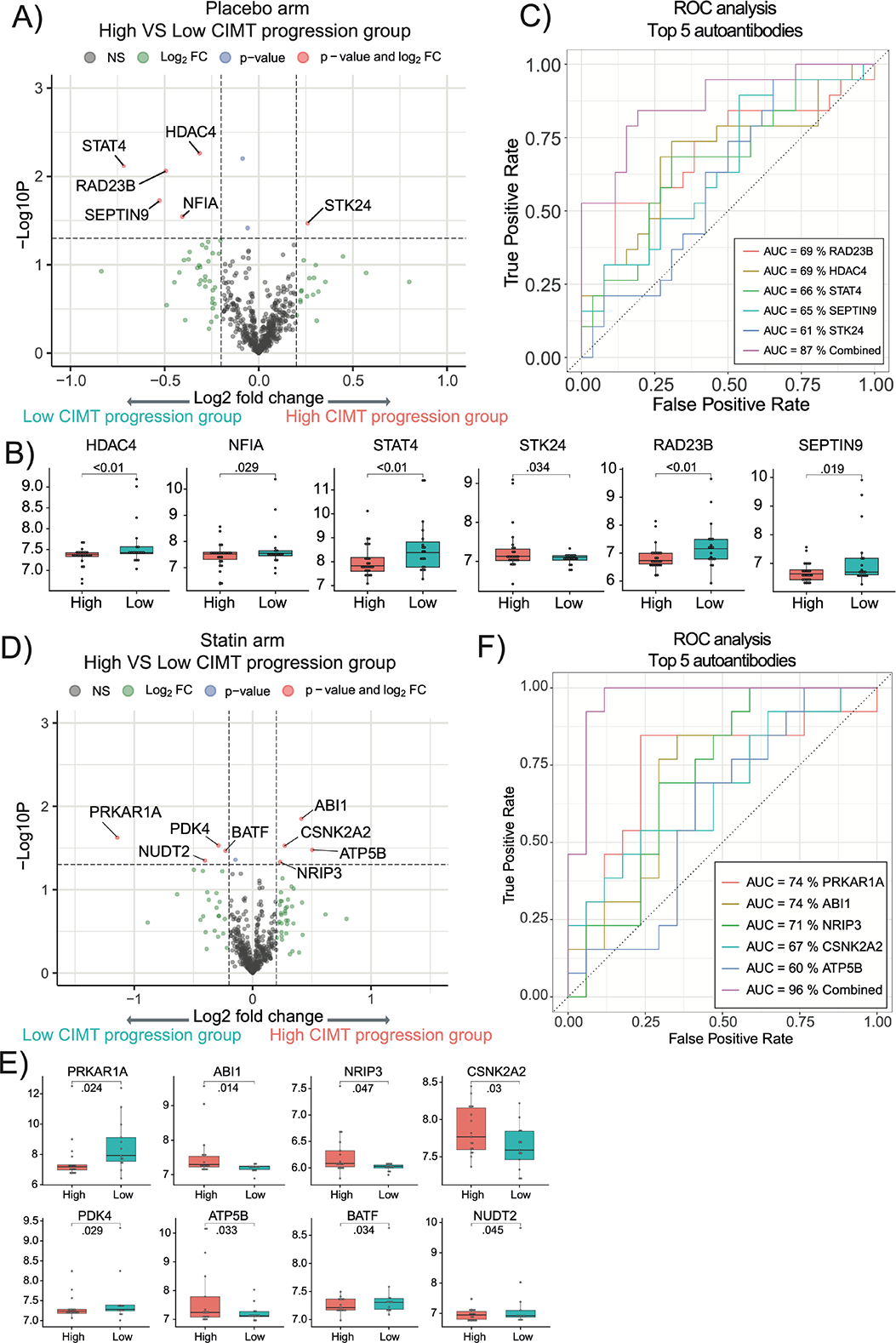
Results: A total of 94 participants (mean [SD] age = 15.3 [2.4] years; 73 [78%] female) recruited to the APPLE trial were included in this biomarker sub-cohort study based on CIMT data and serum sample availability. In the placebo arm, unsupervised clustering analysis of CIMT progression over 3 years identified high (N = 26) and low (N = 19) CIMT progression groups. Similarly, in the atorvastatin arm, a high CIMT progression group (statin non-responders, N = 17) was identified and compared either with the low CIMT progression group (statin responders, N = 13) or with the combined low (N = 13) and intermediate (N = 19) CIMT progression group (defined as responders and partial responders to statin therapy).
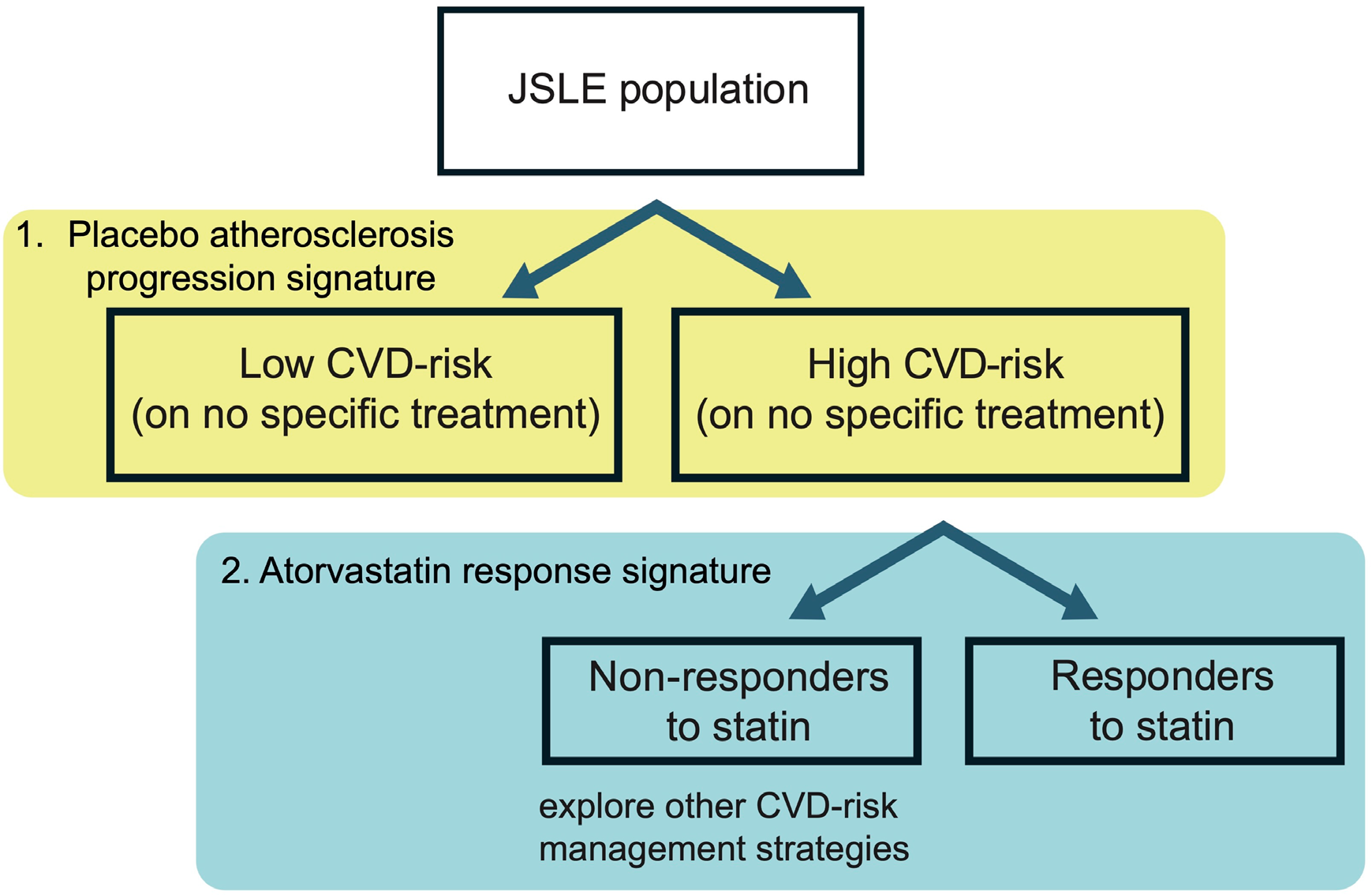
Across all baseline serum samples, 579 autoantibodies were identified as true signals. In the placebo arm, six autoantibodies (STK24, RAD23B, HDAC4, STAT4, SEPTIN9 and NFIA) were significantly associated with high versus low CIMT progression, achieving a combined area under the curve (AUC) of 87% for distinguishing progression patterns (Figure 1A-C). In contrast, a distinct autoantibody profile was identified in the atorvastatin arm: eight autoantibodies (ABI1, ATP5B, CSNK2A2, NRIP3, PRKAR1A, PDK4, BATF and NUDT2) were significantly associated with CIMT progression despite atorvastatin therapy, achieving an exceptional combined AUC of 96% (Figure 1D-F). Pathway enrichment analysis of the statin-associated autoantibody signature suggested lipid-independent mechanisms potentially contributing to persistent atherosclerosis progression in statin-treated patients. Based on the predictive models generated from these distinct autoantibody profiles in both placebo and atorvastatin arms, we propose a two-step stratification strategy using baseline autoantibody profiling to identify (i) individuals at high risk of atherosclerosis progression and (ii) those unlikely to respond to statin therapy, enabling precision-guided CVD risk management in JSLE (Figure 2).
Conclusions: In this biomarker discovery cohort study, novel autoantibody signatures were identified as the first JSLE-specific biomarkers for atherosclerosis progression and prediction of statin response, suggesting possible autoimmune mechanisms underlying the increased CVD risk associated with JSLE. These findings support the potential utility of autoantibody profiling for precision medicine approaches for CVD-risk identification and tailored management in JSLE for ultimate patient benefit.
REFERENCES: [1] Schanberg LE, Sandborg C, Barnhart HX, et al. Premature atherosclerosis in pediatric systemic lupus erythematosus: risk factors for increased carotid intima-media thickness in the atherosclerosis prevention in pediatric lupus erythematosus cohort. Arthritis Rheum . May 2009;60(5):1496-507. doi:10.1002/art.24469.
Acknowledgments: NIL.
Disclosure of Interests: None declared.