fetching data ... 
Background: B cell–mediated autoantibody production is a central pathogenic mechanism in autoimmune diseases (AID), including systemic lupus erythematosus (SLE). Increasing evidence also implicates gut microbiome dysbiosis in the immunopathogenesis of SLE [1]. Autologous CD19 chimeric antigen receptor (CAR) T-cell therapy enables profound B-cell depletion and represents a promising therapeutic strategy for AID. Previous studies have shown that a single infusion of CD19 CAR T-cells is well tolerated in patients with SLE as well as other AIDs, such as systemic sclerosis (SSc) and idiopathic inflammatory myopathy (IIM), and can induce sustained, drug-free remission [2–4]. Given that CD19 CAR T-cell therapy profoundly reshapes adaptive immunity and has been reported to alter serum IgA levels, we sought to investigate its effects on the gut microbiome and fecal IgA.
Objectives: To characterize gut microbiota composition, fecal IgA levels, and anti-commensal bacterial IgA and IgG in patients with AID before and after autologous CD19 CAR T-cell therapy, and to assess their clinical relevance to post-therapy B-cell reconstitution.
Methods: Patients with severe SLE, SSc, or IIM received a single infusion of 1x10 6 / kg body weight autologous CD19 CAR T-cells, manufactured by lentiviral-based transduction of T-cells with a vector encoding a second-generation CAR with a CD19 binder and a 4-1BB costimulatory domain (Zorpocabtagene-autoleucel (Zorpo-cel, MB-CART19.1); Miltenyi Biomedicine). Fecal samples were collected before and 6 months after CD19 CAR T-cell therapy. Bacterial DNA was extracted from the fecal samples. These samples were analysed for gut microbiota composition by metagenomic shotgun sequencing. In addition, fecal IgA content, and anti-commensal bacterial IgA and IgG were analysed by ELISA, as previously described [5]. Twenty patients with autoimmune diseases (9 SLE, 8 SSc, and 3 IIM) were included. Gut microbiota composition and fecal IgA levels were assessed before and 6 months after therapy. Twenty-three age- and sex-matched healthy controls were enrolled.
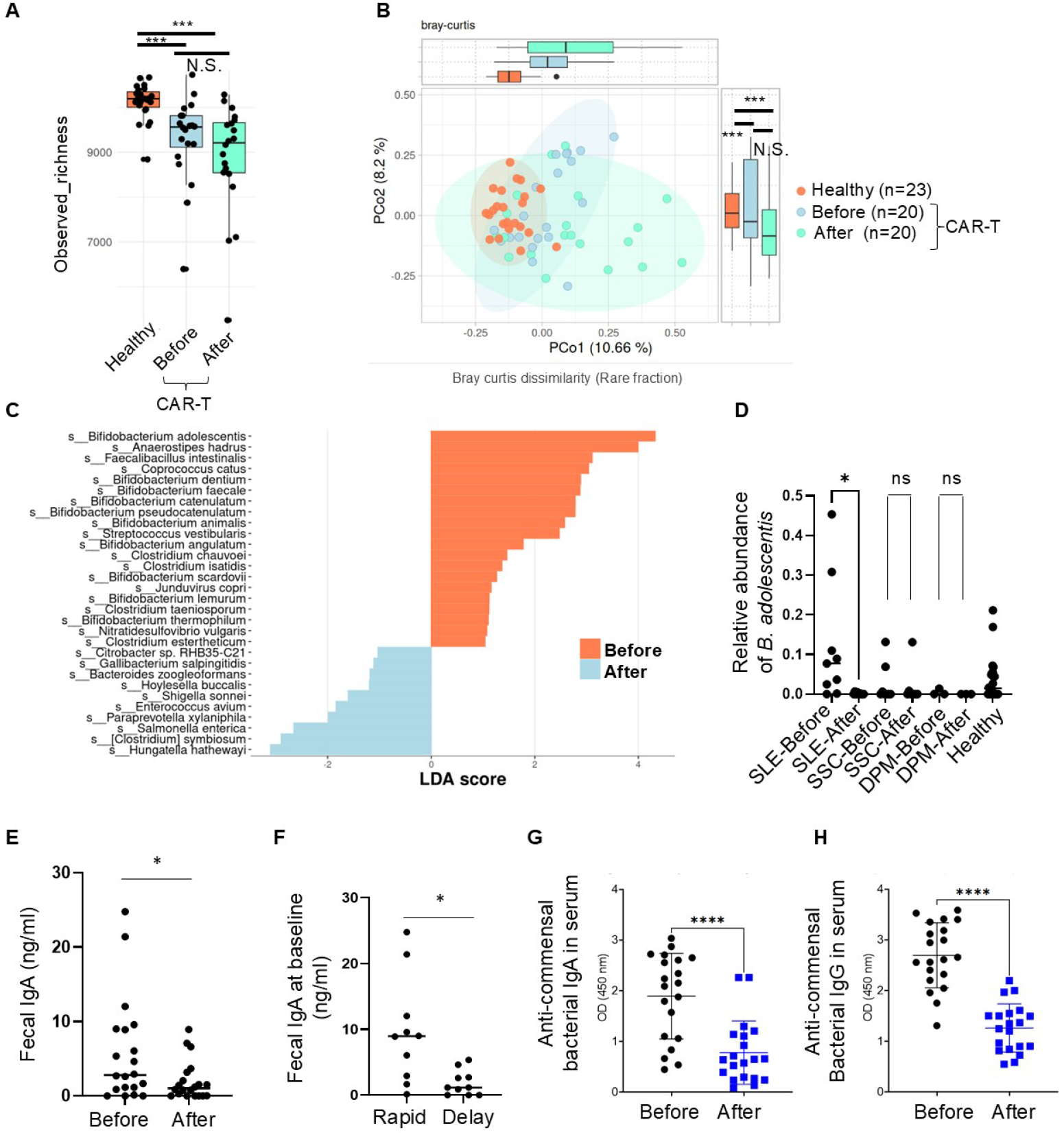
Results: The mean age of patients was 40.7 ± 3.7 years versus 41.2 ± 2.7 years in controls; 11/20 patients and 12/23 controls were female. We first assessed gut microbiota alterations in patients with AID relative to healthy controls. α-diversity was markedly reduced in patients before therapy and remained low 6 months after treatment (Figure 1A). β-diversity analyses demonstrated that microbiota composition in patients, both pre- and post-therapy, differed significantly from controls (Figure 1B). Before CAR T-cell therapy, patients exhibited a significant enrichment of multiple Streptococcus species, consistent with prior reports [6]. LEfSe analysis comparing post- versus pre-therapy samples identified Bifidobacterium adolescentis as the most significantly reduced species after treatment (Figure 1C). This reduction was prominent in patients with SLE but not in those with SSc or IIM (Figure 1D). Mucosal immune activity was evaluated by measuring fecal IgA. Levels were significantly decreased 6 months after therapy (Figure 1E). A subset of patients exhibited delayed CD19 + B-cell reconstitution, defined as failure to recover to >50 cells/µL within 6 months. Patients with delayed recovery had significantly lower baseline fecal IgA levels (Figure 1F), whereas baseline serum IgA, IgG, and gut microbial diversity were not associated with this outcome. These data suggest that reduced mucosal IgA at baseline may predispose to impaired immune reconstitution following CAR T-cell therapy. Finally, anti-commensal bacterial immune responses were examined. Both anti-commensal IgA and IgG levels were significantly reduced 6 months after therapy (Figure 1G, H), indicating a sustained attenuation of humoral immune responses against intestinal bacteria following CAR T-cell treatment.
Conclusions: We show that CD19 CAR T-cell therapy reshapes gut microbiota in patients with AID, prominently reducing B. adolescentis . Notably, B. adolescentis has been shown to promote intestinal Th17 responses, exacerbate experimental arthritis, and impair epithelial barrier function [7–9]. Concurrently, fecal IgA and serum anti-commensal IgA and IgG responses declined. These immunomicrobial shifts may support long-term disease remission. Notably, lower baseline fecal IgA predicted delayed B-cell reconstitution at 6 months, highlighting mucosal immune status as a potential regulator of post–CAR T-cell immune recovery.
REFERENCES: [1] Manfredo Vieira S, Kriegel MA. Science 2018;359:1156–1161.
[2] Mougiakakos D, et al. N Engl J Med 2021;385:567–569.
[3] Mackensen A, et al. Nat Med 2022;28:2124–2135.
[4] Müller F, Taubmann J, Bucci L, et al. N Engl J Med 2024;390:687–700.
[5] Masahata K, et al. Nat Commun 2014;5:3704.
[6] Tomofuji Y, Maeda Y, et al. Ann Rheum Dis 2021;80:1575–1583.
[7] Ang QY, et al. Cell 2020;181:1263–1275.e16.
[8] Tan TG, et al. Proc Natl Acad Sci U S A 2016;113:E8141–E8150.
[9] Bootz-Maoz H, et al. Cell Rep 2022;41:111657.
Acknowledgments: NIL.
Disclosure of Interests: Yuichi Maeda: None declared, Ilia Gimaev: None declared, Sylvio Redanz: None declared, Eva Schmid: None declared, Nadine Otterbein: None declared, Melanie Hagen: None declared, Andreas Wirsching: None declared, Tobias Rothe: None declared, Stefan Wirtz: None declared, Ricardo Grieshaber-Bouyer: None declared, Fabian Müller: None declared, Michael Aigner Miltenyi, Miltenyi, Simon Völkl: None declared, Andreas Mackensen: None declared, Thomas Vogl: None declared, Ilana Brito: None declared, Georg Schett: None declared, Martin Kriegel: None declared, Mario M. Zaiss: None declared.