fetching data ... 
Background: Idiopathic inflammatory myopathies (IIM) are clinically and biologically heterogeneous and are commonly stratified by myositis-specific autoantibodies (MSA) [1]. However, organ damage and treatment responses often transcend MSA classes, indicating additional disease-defining axes. Recent single-cell studies reported expansion of inflammatory classical monocytes expressing IL1B and neutrophil-attracting chemokines in dermatomyositis (DM) [2], yet the genetic and organ-level relevance of this subset across IIM remains unclear.
Objectives: To define pathological mechanisms underlying IIM heterogeneity and muscle damage through integration of genetic risk with peripheral blood and muscle transcriptomic profiles.
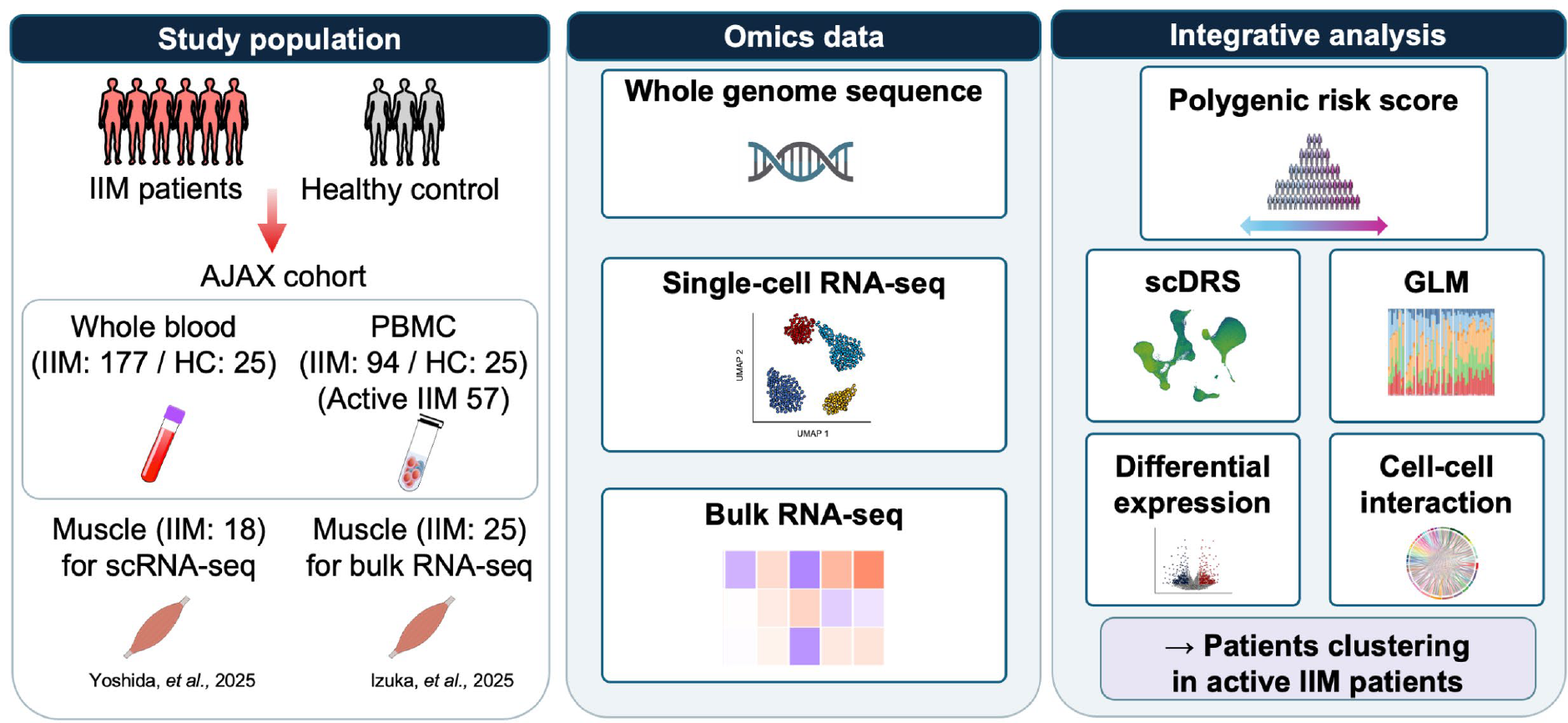
Methods: We enrolled 177 patients with IIM and 25 healthy controls (HC) for whole genome sequencing (WGS). We performed 10x Genomics single-cell RNA sequencing (scRNA-seq) of CD45 + live peripheral blood mononuclear cells (PBMCs) in 94 IIM and 25 HC (approximately 500,000 cells after quality control) ( Figure 1 ). We additionally integrated muscle scRNA-seq from 18 patients and bulk muscle RNA-seq from 25 patients [3] from an independent cohort. Polygenic risk scores (PRS) were calculated using Japanese GWAS summary statistics [4], and GWAS-to-cell-type enrichment was assessed using single-cell disease relevance score (scDRS). Interferon alpha (IFN-α) response module scores were computed across immune subsets. Clinical disease activity was assessed using International Myositis Assessment and Clinical Studies Group (IMACS) core set measures. Associations between cell proportions and clinical measures were tested using generalised linear models adjusted for age, sex, treatment status and MSA. Among untreated or highly active patients at sampling, phenotype-led stratification was performed by principal component analysis of clinical features followed by hierarchical clustering to identify homogeneous clinical groups.
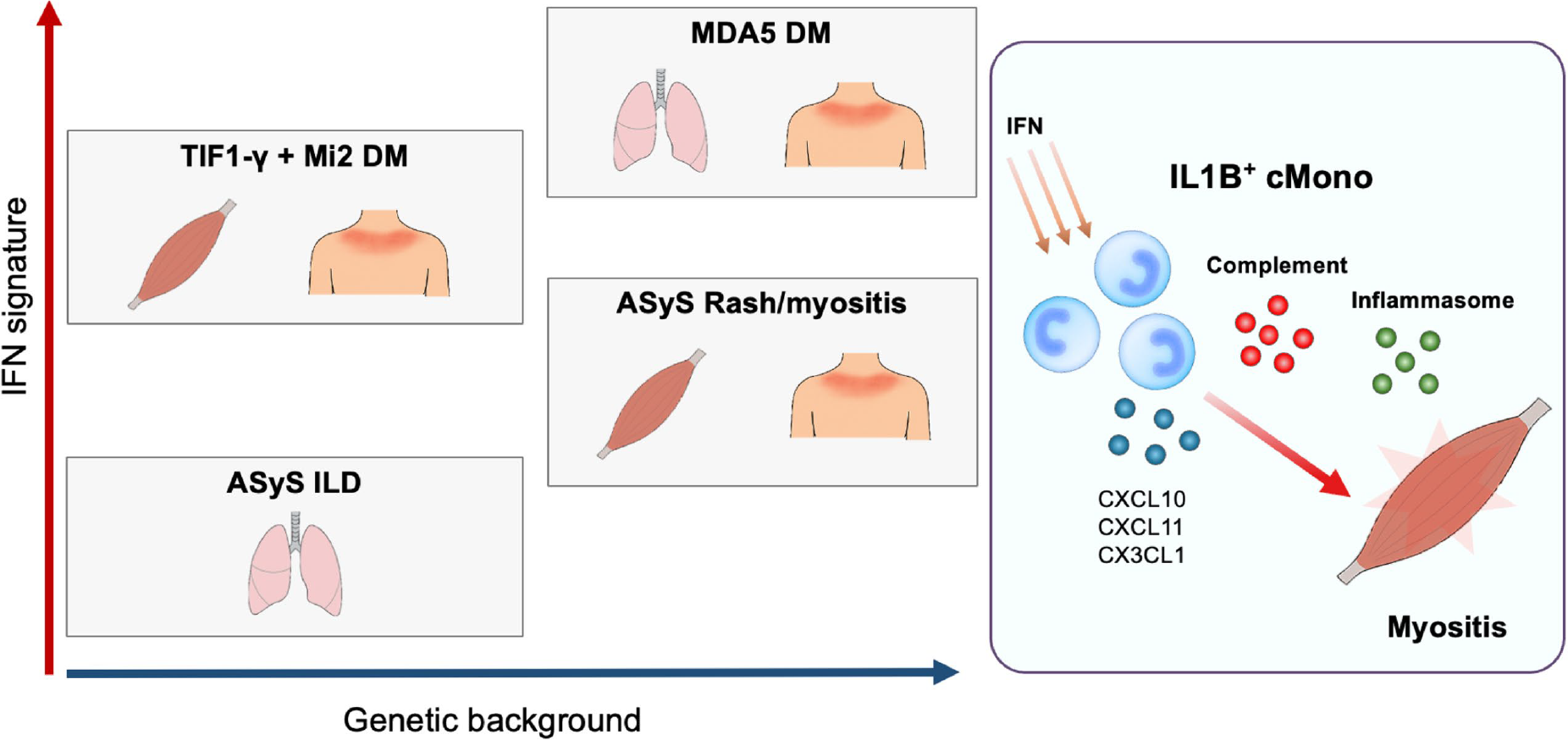
Results: Genetic risk enrichment by scDRS was highest in monocytes, with a marked concentration in IL1B + classical monocytes (cMono) (FDR<0.05). This subset was increased in IIM compared with HC, including in patients classified as clinically inactive at sampling. The proportion of IL1B + cMono was positively associated with patient global assessment, constitutional Myositis Disease Activity Assessment Tool (MDAAT) score, serum creatine kinase and aldolase (P<0.05). Integrated blood and muscle analyses showed selective enrichment of IL1B + cMono in muscle immune infiltrates, with a higher relative abundance in muscle than in PBMCs. Clinical phenotype-led stratification identified four clinical groups: C1 (anti-synthetase syndrome predominant, with mechanic’s hands and interstitial lung disease), C2 (TIF1-γ-positive or Mi-2-positive DM predominant), C3 (MDA5-positive DM predominant), and C4 (anti-synthetase syndrome predominant, with rash and myositis). IL1B + cMono were expanded in all groups versus HC. In contrast, PRS varied across phenotypes: C1 and C2 were comparable to HC, whereas C3 and C4 showed significantly higher PRS (P=0.020 and P=0.017, respectively), suggesting distinct genetic architecture despite shared inflammatory monocyte expansion. IFN-α response module scores in monocyte subsets were highest in C2 and C3, followed by C4, while C1 showed only a modest increase versus HC.
Conclusions: Integrating WGS-derived genetic risk with peripheral and muscle transcriptomics identifies IL1B + cMono as a central cellular axis associated with muscle damage across IIM, including beyond conventional MSA strata. Phenotype-led grouping reveals dissociation between monocyte expansion, interferon signalling, and polygenic burden, generating testable therapeutic hypotheses centred on inflammatory monocytes and context-specific IFN programmes ( Figure 2 ).
Study design and multi-omics integration workflow
Integrated model of IL1B + cMono enrichment, genetic risk, and interferon programmes across IIM phenotypes
REFERENCES: [1] Lundberg IE, Fujimoto M, Vencovsky J, et al. Nat Rev Dis Primers. 2021 Dec 2;7(1):86.
[2] Osborne GA, Zhang L, Ma F, et al. Sci Transl Med. 2025 Dec 24;17(830):eaea9007.
[3] Izuka S, Umezawa N, Komai T, et al. Arthritis Rheumatol. 2025 Jan;77(1):99-106.
[4] Kochi Y, Kamatani Y, Kondo Y, et al. Ann Rheum Dis. 2018 Apr;77(4):602-611.
Acknowledgments: NIL.
Disclosure of Interests: Shinji Izuka Eli Lilly, Eisai, Toshihiko Komai Eli Lilly, AstraZeneca, Tanabe Mitsubishi, Pfizer, AbbVie, Chugai, Daiichi-Sankyo, Eli Lilly, Eisai, Novartis, Taisho Pharmaceutical, Janssen, GlaxoSmithKline, AstraZeneca, Asahi Kasei Pharma, GlaxoSmithKline, Ikuko Ueda: None declared, Manabu Fujimoto Abbvie, Sanofi, Eli Lilly, JBPO, Maruho, Sun Pharma, Taiho Pharma, Novartis, Maruho, Sato Pharma, Hiroyuki Fukui: None declared, Masaru Takeshita: None declared, Natsuka Umezawa Astrazeneca, Novartis, Taisho, AsahiKASEI, Shinsuke Yasuda Otsuka, Abbvie, AsahiKASEI, Astrazeneca, Chugai, Eli Lilly, Mitsubishi-Tanabe, Ono, Otsuka, Stratoimmune, Chugai, ImmunoForge, Novartis, AsahiKASEI, Yuya Kondo: None declared, Isao Matsumoto: None declared, Mitsutaka Yasuda: None declared, Yuichiro Fujieda MBL, Taisho, AstraZeneca, Takeshi Iwasaki: None declared, Akio Morinobu: None declared, Toshio Kawamoto: None declared, Masakazu Matsushita: None declared, Naoto Tamura AstraZeneca, AbbVie, Kissei, AstraZeneca, Otsuka, Asahi Kasei, Ayumi, Hiroshi Nakajima Otsuka, AstraZeneca, GSK, Sanofi, Asahi Kasei, Chugai, Boehringer Ingelheim, Ken Yoshida Astellas, Eisai, Otsuka, Taisho, Takeda, AbbVie, Asahi Kasei, Astellas, Eisai, Boehringer Ingelheim, Chugai, Eli Lilly, JBPO, Otsuka, Taisho, Takeda, Chugai, Takeo Isozaki Taisho, Eli Lilly, Abbvie, Gilead Sciences, Taisho, UCB, Sanofi, Asahikasei, Phizer, Tanabe-Mitsubishi, Novertis, Esai, Eli Lilly, Taisho, Asahikasei, Nobuyuki Yajima: None declared, Akira Yoshida: None declared, Takahisa Gono Asahi Kasei, Astellas, Boehringer-Ingelheim, BMS, Chugai, Eli Lily, Ono, Tanabe-Mitsubishi, Masataka Kuwana Boehringer Ingelheim, BMS, Chugai, Eli Lilly, Amgen, AstraZeneca, Boehringer Ingelheim, GSK, Kissei, MBL, Mitsubishi Tanabe, Mochida, Novartis, Boehringer Ingelheim, MBL, Masanobu Ueno: None declared, Yoshiya Tanaka Chugai, UCB, Abbvie, AstraZeneca, Eli-Lilly, Behringer-Ingelheim, GSK, Eisai, IQVIA, Daiichi-Sankyo, Otsuka, Taisho, Gilead, BMS, Keiichi Sakurai Asahi Kasei, Boehringer Ingelheim, Taisho, Asahi Kasei, Boehringer Ingelheim, Taisho, Janssen, AbbVie, Eli Lilly, AstraZeneca, GSK, Kimito Kawahata: None declared, Yasuyuki Kamata: None declared, Kojiro Sato Taisho Pharmaceutical, Nippon Kayaku, Kyowa Kirin, Pfizer, Chugai Pharmaceutical Co., Ltd., Asahi Kasei Pharma Corporation, Toshihide Mimura Gilead, Novartis, Sandoz, Pfizer, Chugai, Asahikasei Pharma, Otsuka, Gilead, Chugai, Asahikasei Pharma, Akari Suzuki: None declared, Yuta Kochi Daiichi Sankyo, Kazuhiko Yamamoto: None declared, Hayato Yuki: None declared, Takahiro Itamiya Asahi Kasei Corporation, Bristol-Myers Squibb Company, Affiliation with the University of Tokyo Social Cooperation Program funded by Chugai Pharmaceutical Co., Ltd., Mineto Ota MSD, AstraZeneca, Chugai, Calico Life Sciences, GSK, Mochida Memorial Foundation for Medical and Pharmaceutical Research, Astellas, Chugai Foundation for Innovative Drug Discovery, Affiliation with the University of Tokyo Social Cooperation Program funded by Chugai Pharmaceutical Co., Ltd., Tomohisa Okamura Asahi Kasei, BMS, Affiliation with the University of Tokyo Social Cooperation Program funded by Chugai Pharmaceutical Co., Ltd., Keishi Fujio Chugai, Abbvie, Asahikasei Pharma, Bristol Myers, AstraZeneca, Tanabe Mitsubishi, Eisai, Gilead, Eli Lilly, Pfizer, Astellas, Tsumura, Taisho, Daiichi-Sankyo, Novartis, GlaxoSmithKline, Alexion Pharma, Otsuka, Asahikasei Pharma, Novartis, Chugai, Abbvie, Asahikasei Pharma, Bristol Myers, AstraZeneca, Eisai, Tsumura, Taisho.