fetching data ... 
Background: Cutaneous disease is a major driver of morbidity in dermatomyositis (DM). Skin lesions are often chronic, intensely pruritic, and cosmetically disfiguring, leading to substantial physical and psychosocial impairment and diminished quality of life. Standard therapies – including systemic corticosteroids, conventional disease-modifying antirheumatic drugs (DMARDs), and intravenous immunoglobulin – offer incomplete efficacy, are associated with substantial toxicities, and can require complex or burdensome administration regimens. Even with aggressive treatment, clinically meaningful improvement in skin disease can be elusive, underscoring a major unmet need for rapid, effective, and steroid-sparing treatment options for cutaneous DM [1, 2]. Brepocitinib is an investigational, first-in-class, oral, selective inhibitor of TYK2 and JAK1. In an open-label Phase 2 trial in participants with severe, skin-predominant DM (NCT06433999), brepocitinib 30 mg once-daily was associated with rapid improvement in skin disease activity, with clinically meaningful efficacy by Week 4 that increased through Week 12 [3]. In a subsequent Phase 3 trial in adult DM patients with active skin and muscle disease (VALOR; NCT05437263), brepocitinib 30 mg met the primary endpoint and all nine key secondary endpoints [4]. Skin data from the Phase 3 trial thus provides an opportunity to further characterize the speed of onset of clinically meaningful cutaneous responses in DM patients treated with brepocitinib and to further support the rapid and clinically significant improvements observed in the Phase 2 trial.
Objectives: To evaluate early changes (through week 12) in skin disease activity among participants in the Phase 3 VALOR trial.
Methods: VALOR was a 52-week, multicenter, double-blind, placebo-controlled Phase 3 trial conducted at 90 sites across 20 countries that randomized participants with DM 1:1:1 to receive once-daily oral brepocitinib 30 mg, brepocitinib 15 mg, or placebo. Skin disease activity was assessed using the Cutaneous Dermatomyositis Disease Area and Severity Index-Activity (CDASI-A), a validated DM skin-specific tool that assesses the extent and severity of cutaneous disease activity across 15 anatomical locations; scores range from 0-100, with higher scores indicating greater disease severity. CDASI-A response was defined as a both ≥ 40% relative and ≥ 4-point absolute improvement from baseline in CDASI-A, consistent with established clinically meaningful improvement thresholds [4]. Change from baseline in CDASI-A at Week 4 was a ranked key secondary endpoint; the remaining endpoints reported here were prespecified exploratory endpoints. Between-group differences were analyzed using ANCOVA for continuous outcomes and Cochran-Mantel-Haenszel for categorical outcomes.
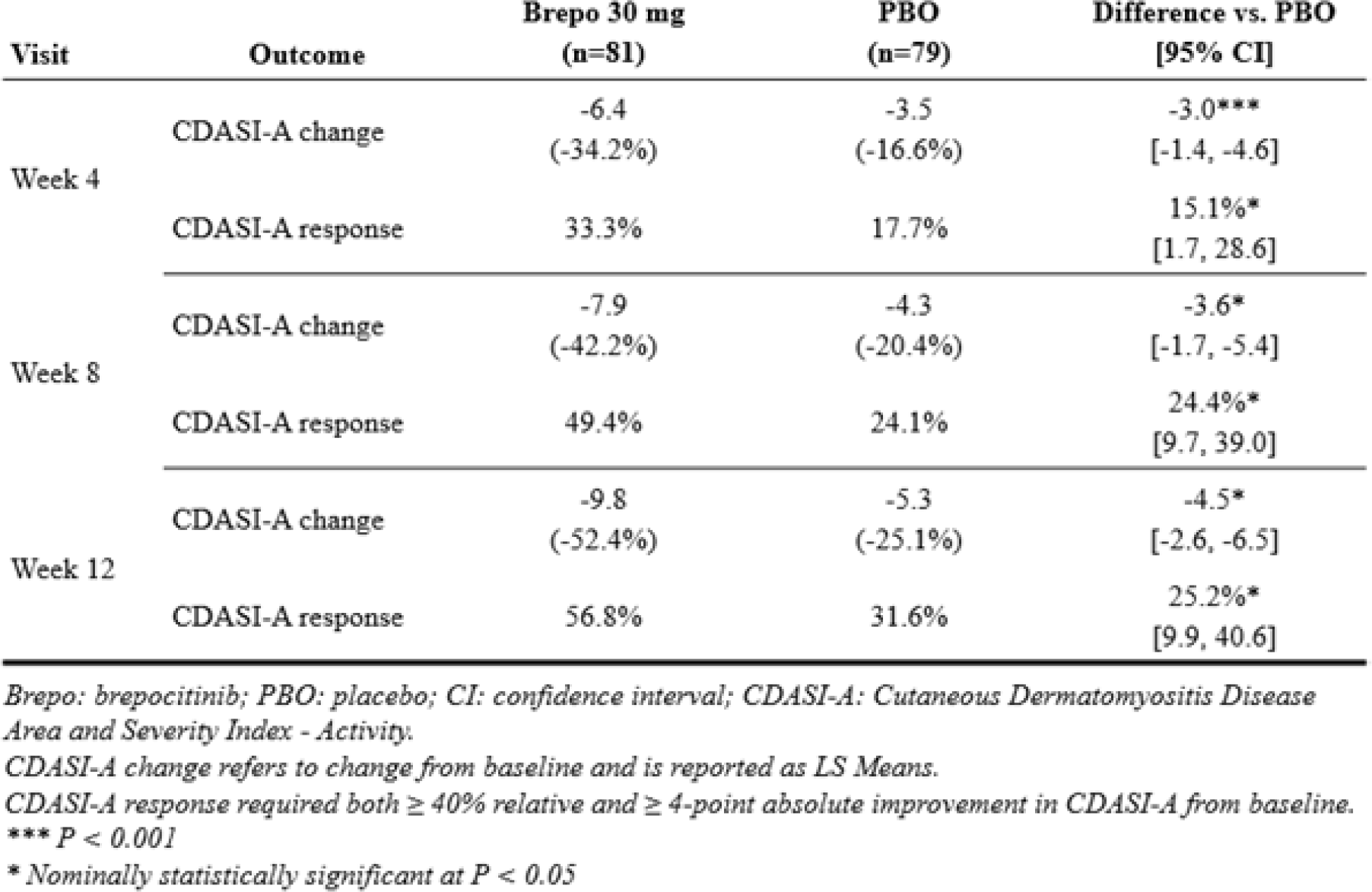
Results: N=241 participants were enrolled. Participants had highly active skin disease at baseline, with a mean CDASI-A score of 19.8; 60.6% had a CDASI-A score of > 14 [5]. The majority of participants (81.3%) were receiving ongoing treatment with two or more standard systemic therapies for DM at baseline. As indicated in Table 1 , brepocitinib 30 mg was associated with rapid, statistically significant, and clinically meaningful benefits on CDASI-A compared to placebo. The key secondary endpoint of change from baseline in CDASI-A at week 4 was met (brepocitinib 30 mg vs. placebo: -6.4 vs. -3.5; treatment difference: -3.0; 95% CI: -1.4 to -4.6; P = 0.0003). Brepocitinib 30 mg was associated with increasing benefit on CDASI-A at weeks 8 and 12, with the mean change at week 12 for brepocitinib 30 mg corresponding to a net 52.4% reduction in CDASI-A from baseline. Brepocitinib 30 mg was also associated with increased achievement of CDASI-A response, with nominal statistical significance achieved at weeks 4, 8, and 12, and high rates of CDASI-A response with brepocitinib 30 mg (49.4% at Week 8; 56.8% at Week 12). Greater benefits were observed with brepocitinib 30 mg among the subgroup of participants with baseline CDASI-A > 14. The efficacy of brepocitinib 30 mg on skin disease activity was sustained during the remainder of the 52-week placebo-controlled period despite greater oral corticosteroid tapering in the brepocitinib 30 mg group relative to placebo. Intermediate effects were observed with brepocitinib 15 mg, indicating a dose-response relationship. Brepocitinib was generally well-tolerated, with a safety profile consistent with approved TYK2 and JAK inhibitors.
Conclusions: Consistent with the results of a prior Phase 2 study in skin-predominant DM, brepocitinib 30 mg once-daily was associated with rapid, clinically significant improvement in skin disease activity in DM. In both trials, clinically meaningful efficacy was observed by Week 4 and increasing benefit was observed through Week 12. Together, these results demonstrate rapid, meaningful benefits of brepocitinib 30 mg on skin disease activity and support brepocitinib as a targeted, potential therapy for patients with DM.
Table 1. CDASI-A Change and CDASI-A Responses Through Week 12 With Brepocitinib 30 mg Versus Placebo
REFERENCES: [1] Cobos G. A, et al. Am. J. Clin. Dermatol. 21; 339–353; 2020.
[2] Wolstencroft P.W, et al. JAMA Dermatol. 2017.
[3] Mangold AR, et al. RDS. 2025.
[3] Paik J. J., et al. J. Invest. Dermatol. 145; 89; 2025.
[4] Anyanwu C.O., et al. Br. J. Dermatol. 2015.
Acknowledgments: NIL.
Disclosure of Interests: Ruth Vleugels: None declared, Elena Schiopu: None declared, Ashley Crew: None declared, Andrea Maderal: None declared, Sheila Shaigany: None declared, Jarad Levin: None declared, Harry Dao: None declared, John Edminister: None declared, Mehdi Rashighi: None declared, Matthew Cascino Priovant Therapeutics, Priovant Therapeutics, Zachary Holcomb: None declared, Margaret Coates: None declared, Astia Allenzara: None declared.