fetching data ... 
Background: Current disease activity assessment in inflammatory myopathies (IIM) relies on serum muscle enzymes and acute-phase reactants, which correlate imperfectly with clinical status and may remain normal despite active disease. Nailfold videocapillaroscopy (NVC) directly visualizes microvascular inflammation, but its utility as an activity biomarker remains unexplored. Traditional subjective NVC interpretation limits clinical applicability.
Objectives: To develop and validate a standardized, automated multiparametric quantitative NVC model for predicting IIM disease activity and to compare its discriminative performance against conventional laboratory biomarkers.
Methods: CAPIAMI is an international multicenter registry enrolling 310 patients with IIM from more than 25 centers across 8 countries and 3 continents. All patients fulfilled 2017 EULAR/ACR classification criteria. This represents the first study employing standardized automated quantitative NVC in IIM, eliminating inter-observer variability through AI-based image analysis. NVC was performed using 200× magnification NVC across 8 nailfold positions per patient. Images were analyzed using Capillary.io AI software, automatically extracting six parameters: (1) capillary density (cap/mm), (2) percentage normal capillaries, (3) percentage megacapillaries, (4) total microhemorrhages, (5) Cutolo pattern classification (normal/early/active/late), and (6) capillary flux. Laboratory biomarkers comprised CPK, LDH, ESR, and CRP. Disease activity was independently assessed by treating physicians using validated clinical criteria. Patients were classified as active (n=232, 74.8%) or inactive (n=78, 25.2%). Five predictive models were developed using multivariable logistic regression: (1) Combined NVC+Laboratory (10 variables), (2) NVC-only (6 variables), (3) Laboratory-only (4 variables), (4) Capillary density alone, and (5) LDH alone. Internal validation employed 1,000-iteration bootstrap resampling. Discriminative capacity was assessed via ROC curve analysis with AUC calculation. DeLong test compared AUCs between models. Statistical significance was set at p<0.05.
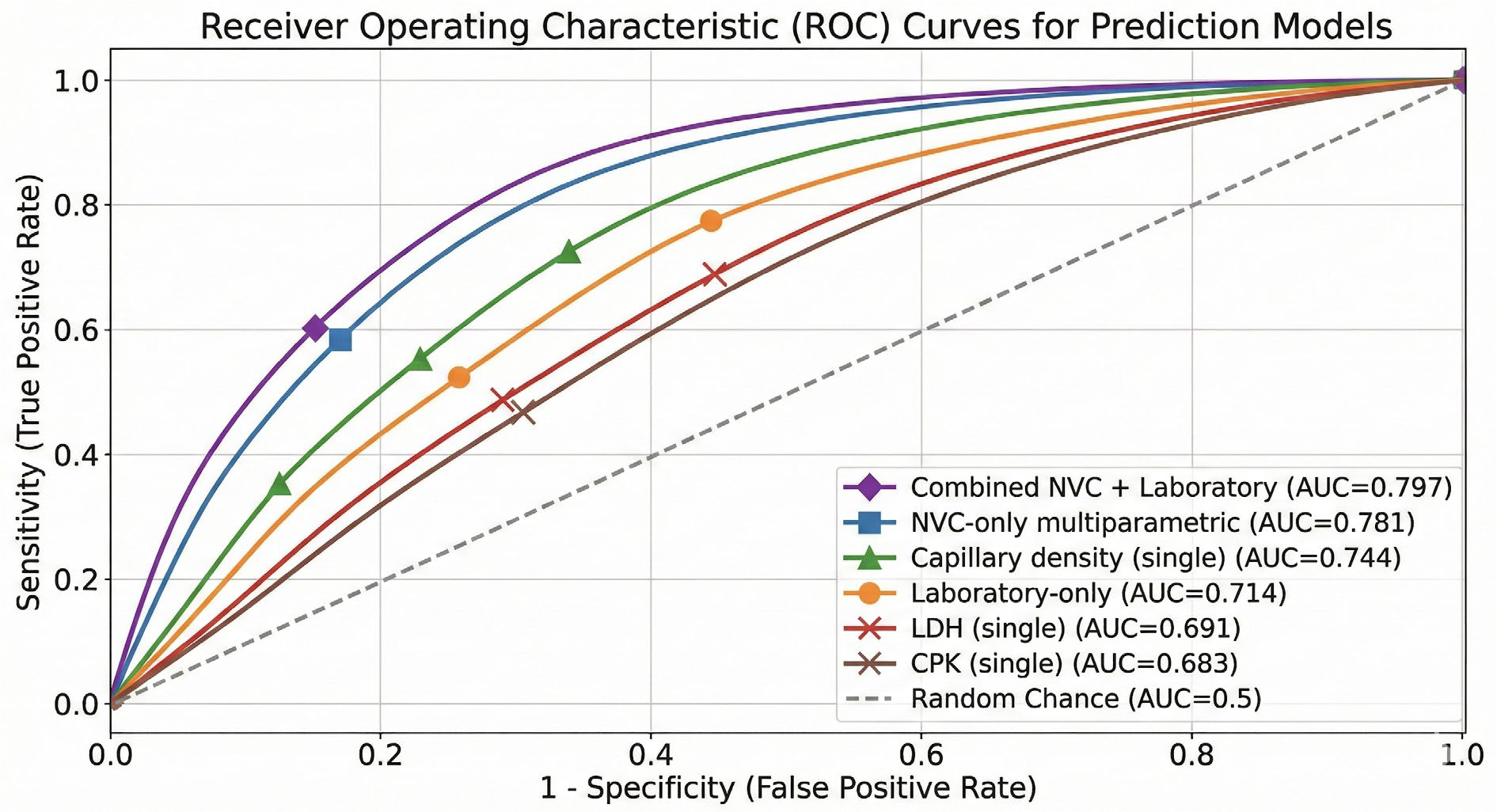
Results: The median age was 57.0 years (IQR 41.0–67.0), and 69.6% were female. Ethnic distribution was 66.4% Caucasian, 19.6% Latin American, 9.6% Amerindian, and 4.3% other groups. Dermatomyositis was the predominant subtype (49.8%), followed by antisynthetase syndrome (18.0%), overlap myopathy (16.1%), immune-mediated necrotizing myopathy (8.5%), and polymyositis (7.5%). Clinically active disease was present in 74.8% of patients. Among patients with active disease, the most frequent manifestations were myositis (63.9%), cutaneous involvement (42.7%), interstitial lung disease (26.4%), articular symptoms (20.3%), and myocarditis (1.8%). The Combined NVC+Laboratory model (10 parameters) achieved the highest discriminative capacity with AUC 0.797 (95% CI 0.75–0.85), significantly outperforming all alternative approaches (Figure 1). At optimal predicted probability threshold (0.70), this model demonstrated sensitivity 60.2%, specificity 83.3%, positive predictive value 91.4%, and negative predictive value 41.7%. Critically, the NVC-only multiparametric model (6 parameters) achieved AUC 0.781 (95% CI 0.73–0.83), significantly superior to the laboratory-only model (CPK, LDH, ESR, CRP; AUC 0.714, 95% CI 0.66–0.77; p=0.008), establishing that quantitative microvascular assessment captures disease activity information independent of, and superior to, systemic inflammatory and muscle enzyme markers. Both single-parameter models performed significantly worse: capillary density alone AUC 0.744 (p=0.046 vs combined) and LDH alone AUC 0.691 (p<0.001 vs combined) (Table 1). Multivariable logistic regression analysis revealed that NVC parameters emerged as the dominant independent predictors. Cutolo pattern (OR 1.95, 95% CI 0.94–4.13, p=0.076) and percentage normal capillaries (OR 1.96, 95% CI 0.97–3.90, p=0.060) demonstrated the strongest associations approaching statistical significance. Conversely, traditional biomarkers contributed minimal independent information beyond other variables: CPK (OR 1.02, 95% CI 0.89–1.15, p>0.85), LDH (OR 0.98, 95% CI 0.85–1.12, p>0.85), ESR (OR 1.01, 95% CI 0.88–1.14, p>0.85), and CRP (OR 0.99, 95% CI 0.87–1.13, p>0.85), with all odds ratios approximating 1.0, confirming their limited utility when combined with quantitative NVC data. Bootstrap internal validation demonstrated stable model performance with minimal overfitting (calibration slope 0.92).
Conclusions: Automated quantitative NVC provides superior discrimination of IIM disease activity compared to standard serum biomarkers. With a PPV >91%, quantitative NVC effectively “rules in” active disease, supporting confident treatment intensification even when enzymes are equivocal. These findings advocate for a paradigm shift toward integrating automated microvascular imaging into routine IIM monitoring algorithms.
ROC Curves Comparing Predictive Models for Disease Activity in IIM
Predictive Performance of Quantitative NVC and Laboratory Biomarker Models for IIM Disease Activity
| Prediction Model | N Parameters | AUC (95% CI) | Sensitivity (%) | Specificity (%) | PPV (%) | NPV (%) | p vs Combined |
|---|---|---|---|---|---|---|---|
| Combined NVC + Laboratory | 10 | 0.797 (0.75-0.85) | 60.2 | 83.3 | 91.4 | 41.7 | Reference |
| NVC-only multiparametric | 6 | 0.781 (0.73-0.83) | 58.5 | 81.8 | 89.7 | 40.3 | 0.247 |
| Capillary density (single ) | 1 | 0.744 (0.69-0.80) | 54.7 | 77.9 | 86.2 | 38.4 | 0.046 |
| Laboratory-only | 4 | 0.714 (0.66-0.77) | 52.1 | 75.2 | 84.1 | 36.8 | 0.008 |
| LDH (single ) | 1 | 0.691 (0.63-0.75) | 48.3 | 71.4 | 80.5 | 34.1 | <0.001 |
| CPK (single ) | 1 | 0.683 (0.62-0.74) | 45.8 | 69.7 | 78.9 | 33.2 | <0.001 |
REFERENCES: [1] Mugii N, Hasegawa M, Matsushita T, et al. Association between nail-fold capillary findings and disease activity in dermatomyositis. Rheumatology (Oxford ). 2011;50(6):1091-1098.
[2] Torres-Ruiz J, Pinal-Fernandez I, Selva-O’Callaghan A, et al. Nailfold capillaroscopy findings of a multicentric multi-ethnic cohort of patients with idiopathic inflammatory myopathies. Clin Exp Rheumatol . 2024;42(2):367-376.
Acknowledgments: NIL.
Disclosure of Interests: None declared.