fetching data ... 
Background: Inclusion body myositis (IBM) is the most common acquired muscle disease in individuals over the age of 50 and is characterized by a combination of inflammatory and degenerative changes affecting skeletal muscle. IBM is the only idiopathic inflammatory myopathy (IIM) subtype which affects more males than females. Although several human leukocyte antigen alleles have been associated with IBM, the genetic risk factors remain largely unknown. The contribution of sex chromosomes towards the atypical male sex bias observed in IBM is an underexplored hypothesis. One way of investigating the contribution of sex chromosomes in disease is by quantifying the rate of sex chromosome aneuploidies – genetic conditions caused by extra or missing X or Y chromosomes – amongst patients. Previously, a study performed such analyses in IBM and found an increased rate of Klinefelter syndrome (47,XXY) within a cohort of 147 males with IBM compared to the general male population, suggesting that X chromosome dosage may be a genetic risk factor for disease [1]. In addition to sex chromosome aneuploidies that are present from birth, acquired genetic changes known as mosaic chromosomal alterations (mCAs) could contribute to the male sex bias in IBM. mCAs include deletion, duplication or copy-neutral loss of heterozygosity events that are found in a subset of somatic cells in an individual. The most common mCA in males is mosaic loss of Y chromosome (mLOY); the partial or complete deletion of the Y chromosome in a subset of cells. The proportion of males carrying mLOY increases with age and is associated with increased risk of cancer, neurodegenerative diseases, and cardiovascular diseases. A recent study reported that mLOY increased significantly in individuals with late-onset, but not young-onset, rheumatoid arthritis, highlighting a potential role in autoimmunity [2].
Objectives: In this study, we aimed to validate the increased rate of sex chromosome aneuploidies in IBM and analyse the frequency of mosaic loss of X (mLOX) and mLOY in a large cohort of IBM patients using genotype array data collected by The International IBM Genetics Consortium.
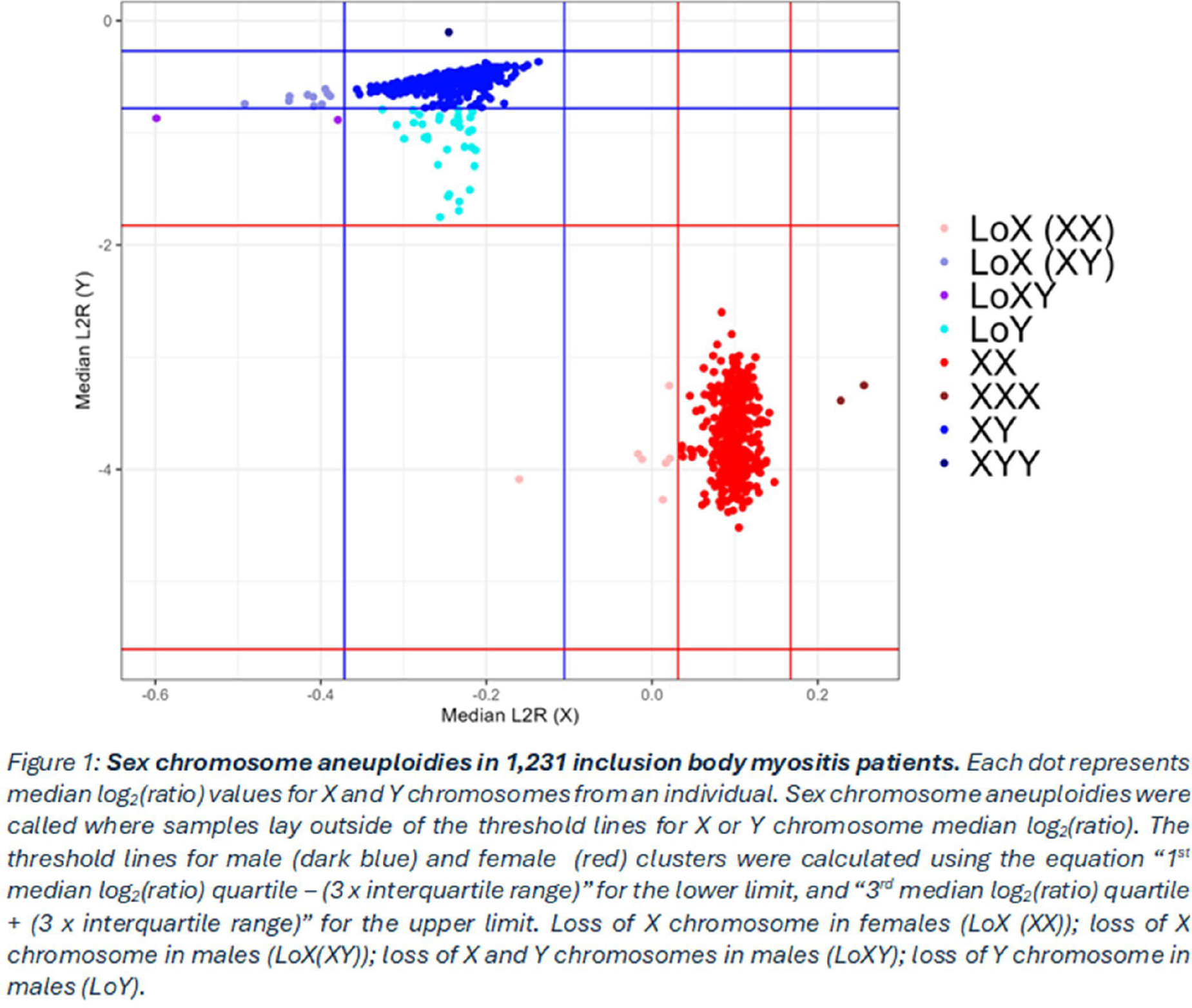
Methods: The International IBM Genetics Consortium collected blood DNA samples from individuals diagnosed with IBM fulfilling Griggs criteria (1995) [3] or the European Neuromuscular Centre criteria 2013 [4]. Initially, the presence of sex chromosome aneuploidies was investigated in 1,231 individuals from The International IBM Genetics Consortium. For this, median log 2 (ratio) (L2R) values for X and Y chromosomes were extracted from genotype array raw intensity data (IDAT) files per individual. Median L2R values for the X and Y chromosomes were plotted against each other for each individual. For male and female clusters, median L2R thresholds were defined using interquartile range values. Samples plotted outside of these thresholds for either sex cluster were determined to harbour sex chromosome aneuploidies. Subsequently, the occurrence of mCA in sex chromosomes was evaluated in 1,119 individuals from The International IBM Genetics Consortium. After variant and sample quality control, genotypes underwent phasing and MoChA tool [5,6] was used to detect mCA, following recommended cut-offs.
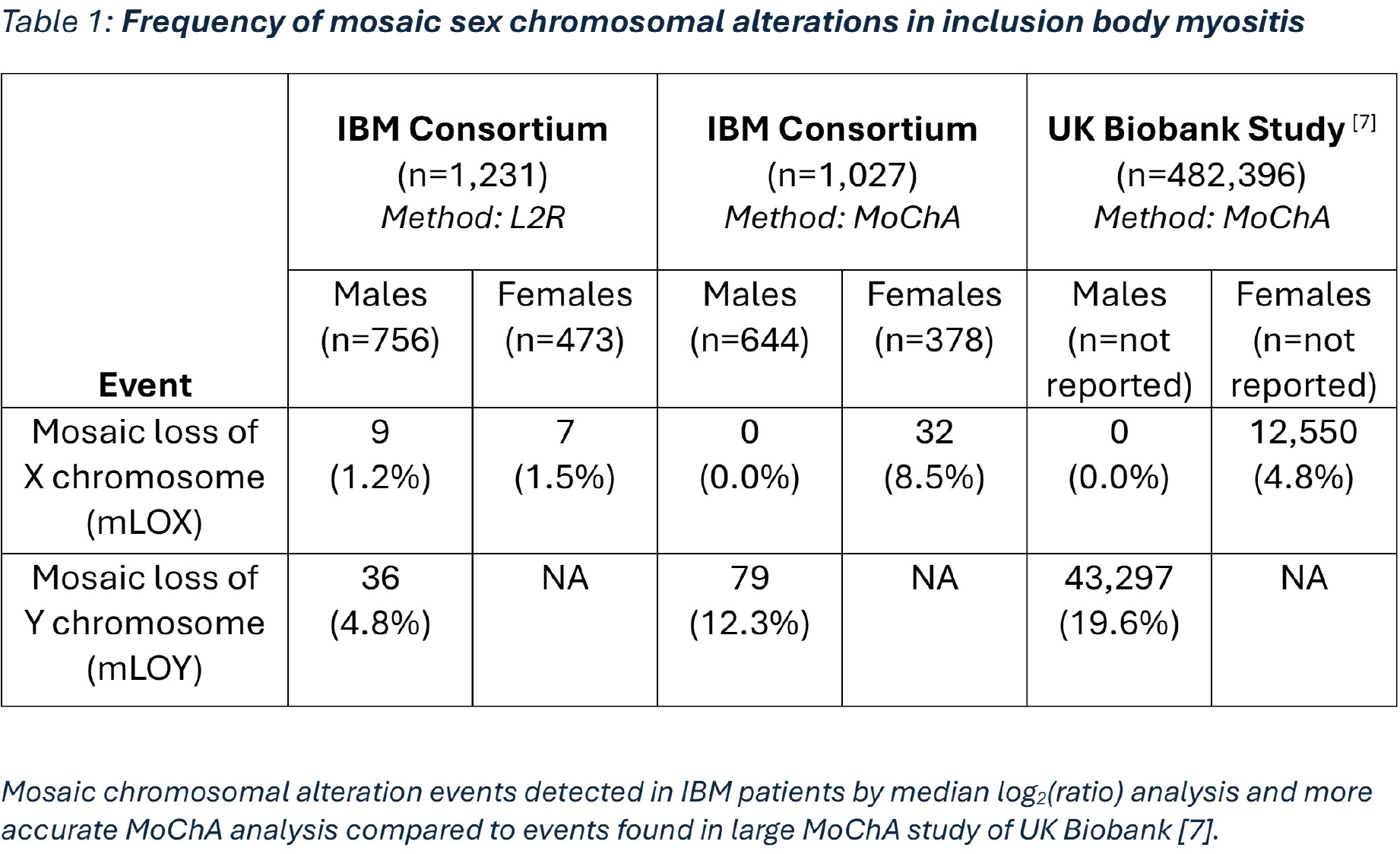
Results: Based on L2R thresholds, no males (0/756) with IBM were identified as possessing Klinefelter syndrome (47,XXY) in contrast to previous studies. One male was identified with possible 47,XYY, and two females (2/473) with 47,XXX. Interestingly, 4.8% of males (36/756) were estimated to harbour loss of Y chromosome (Figure 1). To more accurately characterise the nature of loss of Y in males, mCA detection was performed on 1,119 subjects from The International IBM Genetics Consortium. mCA detection results for 92 subjects failed quality control, so were excluded from analysis. Through this more accurate method, mLOY was detected in 12.3% of IBM males, whilst mLOX was detected in 8.5% of IBM females, compared to 19.6% of males and 4.8% of females from the UK Biobank population (Table 1) [7]. Age information was only available for a subset of IBM males (n=125) subject to mCA detection. Within this subset, males with mLOY were significantly older than males without mLOY (Wilcoxon, p=0.005), and the proportion of males with mLOY tended to increase with age.
Conclusions: This study was the largest investigation into sex chromosome genetics in IBM to date and the first to detect sex chromosome mCAs in individuals with IBM. We found no association between sex chromosome aneuploidies and IBM. The proportion of IBM females with mLOX tended to be greater than that in the general population, whilst proportion of IBM males with mLOY tended to be lower. Future work will validate this study in IBM patient cohorts with greater coverage of demographic information.
REFERENCES: [1] Scofield, R. H., et al. (2022). ‘47XXY and 47XXX in Scleroderma and Myositis’ ACR Open Rheumatol , 4 (6), pp. 528-533.
[2] Uchiyama, S., et al. (2025). ‘Mosaic loss of chromosome Y characterises late-onset rheumatoid arthritis and contrasting associations of polygenic risk score based on age at onset’ Ann Rheum Dis , 84 (8), pp. 1313-1323.
[3] Griggs, R. C., et al. (1995). ‘Inclusion body myositis and myopathies’ Ann Neurol , 38 (5), pp. 705-13.
[4] Rose, M. R. and Group, E. I. W. (2013). ‘188th ENMC International Workshop: Inclusion Body Myositis, 2-4 December 2011, Naarden, The Netherlands’ Neuromuscul Disord , 23 (12), pp. 1044-55.
[5] Loh, P. R., et al. (2018). ‘Insights into clonal haematopoiesis from 8,342 mosaic chromosomal alterations’ Nature , 559 (7714), pp. 350-355.
[6] Loh, P. R., Genovese, G. and McCarroll, S. A. (2020). ‘Monogenic and polygenic inheritance become instruments for clonal selection’ Nature , 584 (7819), pp. 136-141.
[7] Lin, S. H., et al. (2021). ‘Incident disease associations with mosaic chromosomal alterations on autosomes, X and Y chromosomes: insights from a phenome-wide association study in the UK Biobank’ Cell Biosci , 11 (1), p. 143.
Acknowledgments: NIL.
Disclosure of Interests: Luke Tomlinson: None declared, David Scannali: None declared, James Eales: None declared, Nathan Routledge: None declared, Alaa Khan: None declared, Iwona Skorupinska: None declared, Conceição Bettencourt: None declared, Jana Vandrovcova: None declared, Sara Nagy: None declared, Michael Sinnreich: None declared, Qiang Gang: None declared, Christina Liang: None declared, Jerome Coudert: None declared, Merrilee Needham: None declared, Jan De Bleecker: None declared, Boel De Paepe: None declared, Willem De Paepe: None declared, Jonathan Baets: None declared, Edmar Zanoteli: None declared, Damien Amelin: None declared, Chrysa Chrysovitsanou: None declared, Miren Zulai: None declared, Marina Mora: None declared, Angelini Corrado: None declared, Michela Ripolone: None declared, Diego Lopergolo: None declared, Anders Oldfors: None declared, Ambreen Tariq: None declared, Aleksandar Radunovic: None declared, Kathryn Walker: None declared, Stefen Brady: None declared, James B. Lilleker JBL has received conference/travel support and speakers fees from Sanofi. He has participated in advisory boards, received conference/travel support and speakers fees from Roche. He has received speakers fees from Dyne therapeutics., Dawn Caraballo: None declared, Anthony Amato: None declared, Thomas Llyod: None declared, Perry Shieh: None declared, Brianna Blume: None declared, Matthew P. Wicklund: None declared, Richard J. Barohn: None declared, Jeffrey Guptill: None declared, Linda Carter: None declared, Elie Naddaf: None declared, Aziz Shaibani: None declared, Heidi Runk: None declared, Mazen Dimachkie: None declared, Amy Bartlett: None declared, John Kissel: None declared, Marinos Dalakas: None declared, Tahseen Mozaffar: None declared, Namita A. Goyal: None declared, Olimpia Carbunar: None declared, Conrad C. Weihl: None declared, Andrew B. Singleton: None declared, Michael G. Hanna: None declared, Henry Houlden: None declared, Pedro M Machado: None declared, Hector Chinoy Yes, Pfizer, Eli-Lilly, AstraZeneca and Janssen., Janine Lamb Yes, Pfizer and Eli-Lilly., GEORGE PAPADIMAS: None declared, Constantinos PAPADOPOULOS: None declared.