fetching data ... 
Background: In rheumatoid arthritis (RA), sustained adherence to disease-modifying antirheumatic drugs (DMARDs) is essential to achieve treatment targets and prevent disease progression; however, adherence remains suboptimal [1]. Few interventions exist to improve DMARD adherence in RA, and these are limited by weak methodological quality, a restricted range of behaviour change techniques (BCTs) used and poor translation into real-world clinical settings [2].
Objectives: To describe the development and characteristics of the SQUEEZE eHealth-facilitated integrated care model (eSCM), designed to improve DMARD adherence in adults with RA and to be pilot-tested and implemented in two Swiss centres.
Methods: Grounded in the eHealth-Enhanced Chronic Care Model [3], the eSCM was developed using an interdisciplinary approach integrating clinical and patient experiences with implementation and behavioural sciences. Stakeholder involvement was guaranteed through iterative co-creation by researchers, clinicians, IT developers and patient research partners. Medication adherence was conceptualised according to the ABC taxonomy, encompassing initiation (first dose taken), implementation (following the regimen) and persistence (from first dose until discontinuation) [4], which guided the identification of target behaviours across the DMARD treatment trajectory. Intervention development followed the Behaviour Change Wheel (BCW ) approach [5] and integrated evidence from:
Systematic review of DMARD adherence interventions;
Findings of the contextual analysis in RA;
Existing real-world RA care models; and
Medication Adherence Promotion System (MAPS) intervention, a real-world adherence intervention with demonstrated clinical effectiveness in transplant care [6, 7].
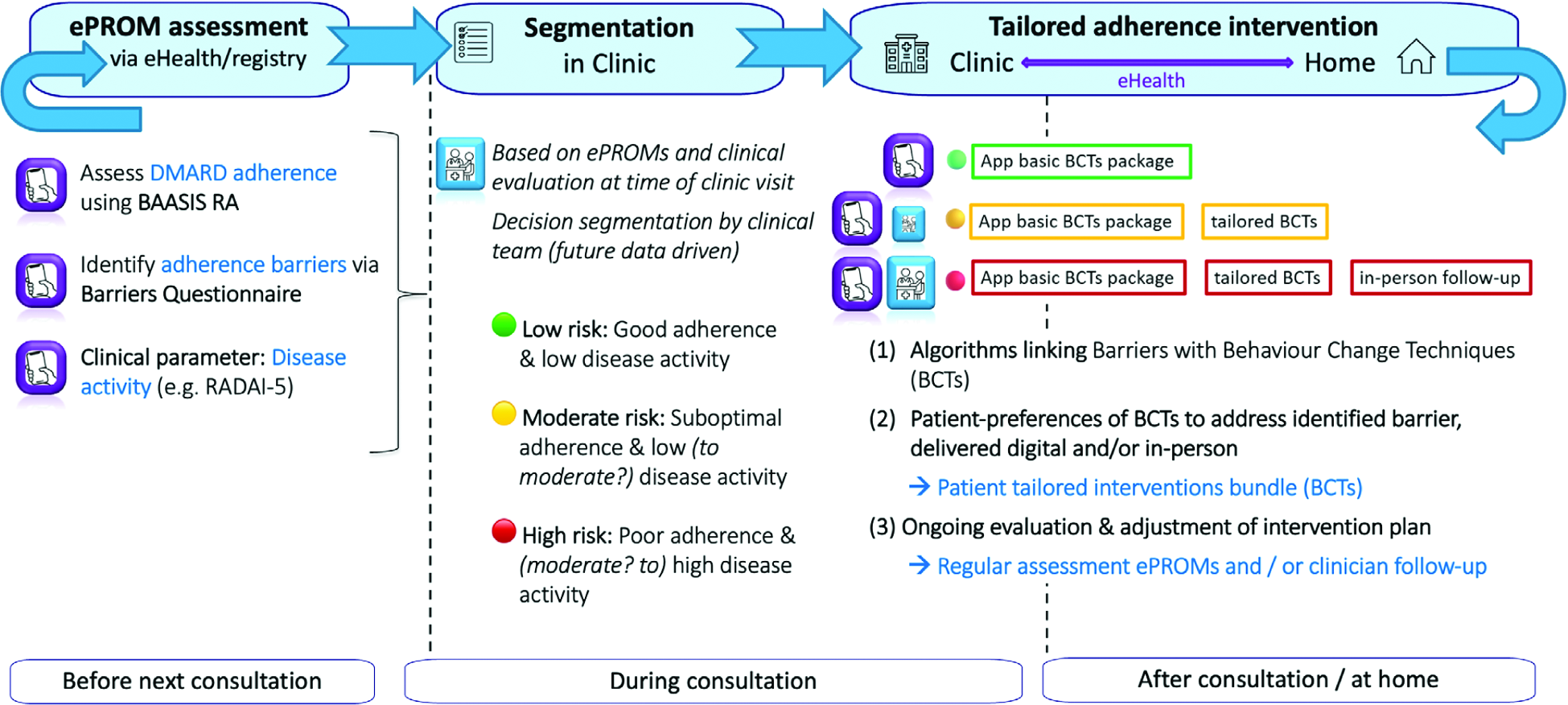
Results: Using the BCW, five key target behaviours related to DMARD implementation and persistence adherence were identified. Multilevel barriers to DMARD adherence were found at the patient level (e.g. experienced or anticipated side-effects, forgetfulness), healthcare practice level (e.g. limited routine adherence monitoring, time constraints), and health system level (e.g. insurance approval delays). These barriers were systematically mapped to the Theoretical Domains Framework aligned with the COM-B model to establish a comprehensive behavioural diagnosis, revealing deficits in psychological and physical capability, reflective and automatic motivation, and social and physical opportunity. Based on this mapping, relevant BCW intervention functions (i.e. education, enablement, persuasion and environmental restructuring) were selected and operationalised through evidence-based BCTs to address frequently occurring and modifiable barriers. The resulting theoretical description of the eSCM, designed for integration into routine care and structurally inspired by MAPS [6, 7], consists of three sequential core components (Figure 1): (1) Risk assessment (pre-clinic visit) using home-based electronic patient-reported outcome measures (ePROMs), to be integrated into the Swiss Clinical Quality Management (SCQM) registry, a nationwide RA registry capturing longitudinal clinical and patient-reported data. Within SCQM, ePROMs will include newly developed tools assessing DMARD adherence via BAASIS-RA (adapted BAASIS [8]) and adherence barriers , alongside routinely collected clinical parameters (e.g., RADAI-5). (2) Segmentation (in clinic), whereby a decision tree algorithm integrates ePROM-based risk assessments with in-person collected clinical data (e.g., DAS28) to segment patients into low, moderate or high adherence-risk categories, with final decisions informed by clinical judgement. (3) Tailored adherence intervention (in clinic/at home) linking patient’s individual barriers to algorithm-driven interventions packages composed of evidence-based BCTs, tailored through shared decision-making to individual needs and preferences. Low-risk patients receive a basic app-based intervention to support sustained adherence, while moderate- and high-risk patients additionally receive personalised, preference-based BCT packages delivered digitally, remotely or in-person, with in-person follow-up prioritised for high-risk patients. Adherence risk assessment and segmentation allow clinicians to prioritise patients in greatest need, saving time. Digital delivery provides patients with tools to self-manage adherence. Regular reassessment via ePROMs (every three months) enables dynamic follow-up and adaptation to evolving adherence risk. Centre-specific implementation strategies support real-world integration of the eSCM into routine care.
Conclusions: The eSCM employs a rigorous methodological foundation grounded in behavioural and implementation science, informed by multiple sources, particularly MAPS evidence. This approach strengthens theoretical rigor while enhancing real-world applicability through continuous stakeholder engagement. This positions the eSCM as a promising adherence model for real-world implementation in routine rheumatology practice. Next, the model will be evaluated in a hybrid pilot study assessing both effectiveness and implementation outcomes in two RA clinics in Switzerland.
Joint senior authorship is shared by the last two authors.
The SQUEEZE eHealth facilitated integrated care model (eSCM )
REFERENCES: [1] Ritschl V. et al., RMD Open, 2020. 6:e001432
[2] Ribaut J. et al., Ann Rheum Dis, 2025. 84: p.1469.
[3] Gee P.M. et al., Med Internet Res, 2015. 17(4): p.e86.
[4] Vrijens B. et al., Br J Clin Pharmacol, 2012. 73(5): p.691-705.
[5] Michie S. et al., Implement Sci, 2011. 6: p.42.
[6] Hooper D.K. et al., Am J Kidney Dis, 2022. 79(3): p.335-346.
[7] Varnell C.D. et al., Am J Kidney Dis, 2022. 80(3): p.330-340.
[8] Denhaerynck K. et al., Transplantation, 2023. 107(8): p.1795-1809.
Acknowledgments: NIL.
Disclosure of Interests: Sofia Calado: None declared, Christina Wettengl: None declared, Janette Ribaut: None declared, Bart van den Bemt: None declared, Simone Brand: None declared, Loreto Carmona: None declared, Kristina Chingov: None declared, Mary Louise Daly CSL, GSK, Biotest, Andreas Dam HealthBuddy P/S – a digital health/therapeutics company (not pharmaceutical), Codruta Zabalan: None declared, Estíbaliz Loza: None declared, Chrysoula Manolaraki: None declared, Teresa Oton: None declared, Diego Kyburz Abbvie, Janssen, Novartis, UCB, Eli Lilly, Pfizer, Sanofi, Abbvie, UCB, Janssen, Sabina De Geest Roche, Novartis, Abbvie, Sanofi, Roche, Novartis, Sanofi, Agnes Kocher Abbvie, Novartis, Pfizer, Boehringer Ingelheim.