fetching data ... 
Background: Juvenile psoriatic arthritis (JPsA) presents with a wide variety of joint involvement and extra-articular features manifesting at different times in the disease course, with varying treatment response to therapies. These imply the presence of biologically distinct disease subsets that could be used to form the basis of a stratified treatment programme. A challenge in identifying such subgroups is the existence of multiple methods to identify JPsA, including the use of multiple classification criteria sets and clinical diagnoses. In addition, existing subgrouping has relied on broad age categories rather than empirical clinical patterns, limiting their ability to guide precision treatment. Modern machine learning approaches and harmonised data sources now enable discovery of such subgroups.
Objectives: i) To identify novel, phenotypically consistent and clinically distinct subgroups of children and young people with JPsA in early disease, ii) To understand how subgroups differ across JPsA identification frameworks.
Methods: Children and young people were selected if enrolled to one of five multicentre inception/population cohorts of JIA: CAPS (UK), ICON (Germany), NPRD (Germany), ReACCh-Out (Canada) or CAPRI (Canada) between January 2001 and December 2023 with a physician’s diagnosis of JPsA, enthesitis-related or undifferentiated JIA. Cohort follow-ups within the first 24 months following symptom onset were used to identify clusters of children with distinct cumulative disease burden within this time frame. Clustering was undertaken in three groups of children who i) fulfilled ILAR criteria for JPsA, ii) had a physician’s diagnosis of JPsA iii) fulfilled CASPAR criteria for PsA. Latent class analysis was used to cluster children using a combination of an active joint count and the presence of psoriasis, dactylitis, and nail abnormalities. Optimal models were selected based on model fit (BIC, likelihood ratio testing) and clinical plausibility, with any model separating a group with <5% of the cohort excluded. Univariable statistics (Kruskal-Wallis, Chi-squared testing) compared outcomes within 24 months and both demographic (age, gender, family history of psoriasis in a first degree relative) and disease characteristics (presence of enthesitis, JIA core outcome variables, ANA positivity) at first available observation following symptom onset across clusters.
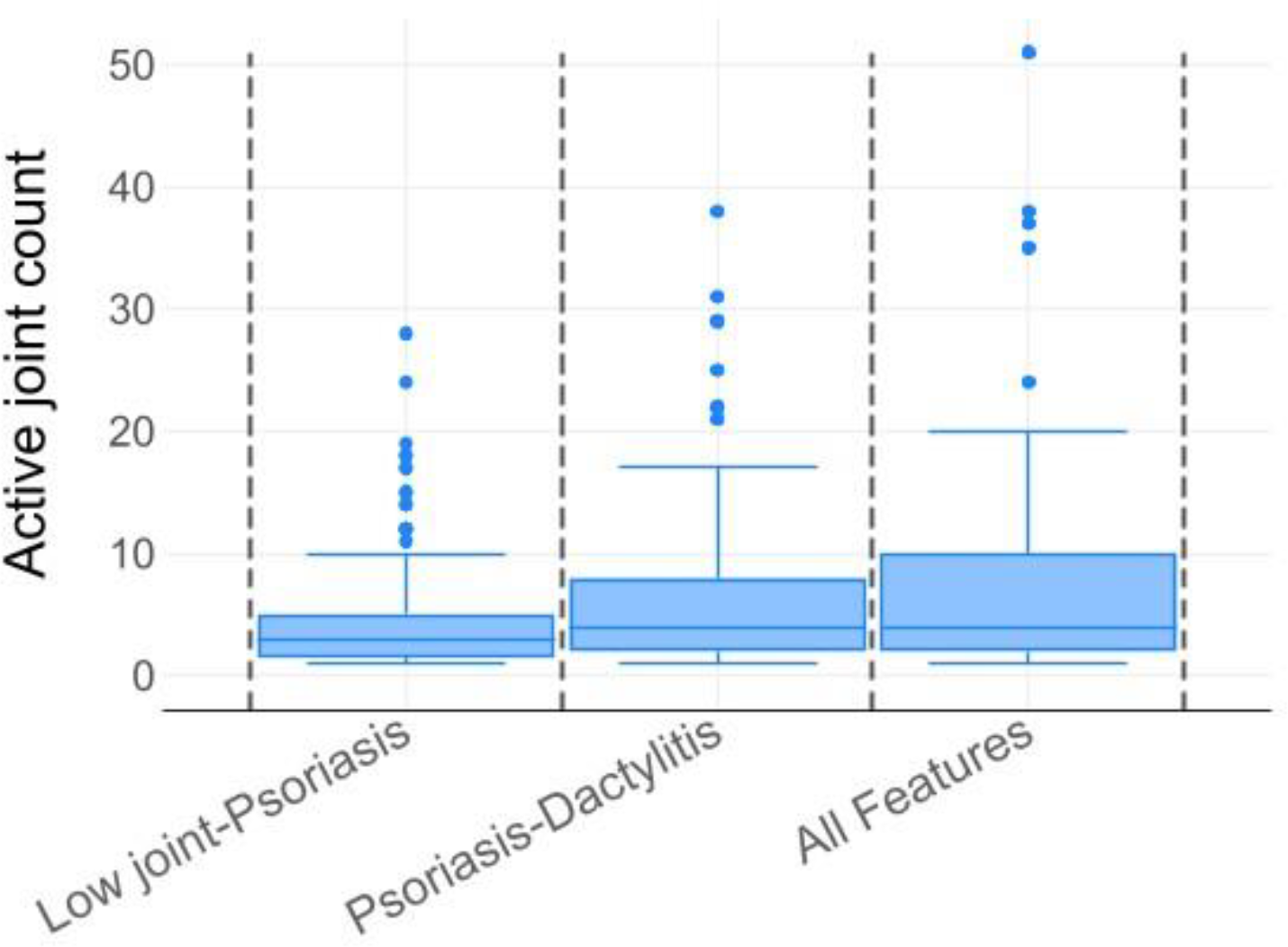
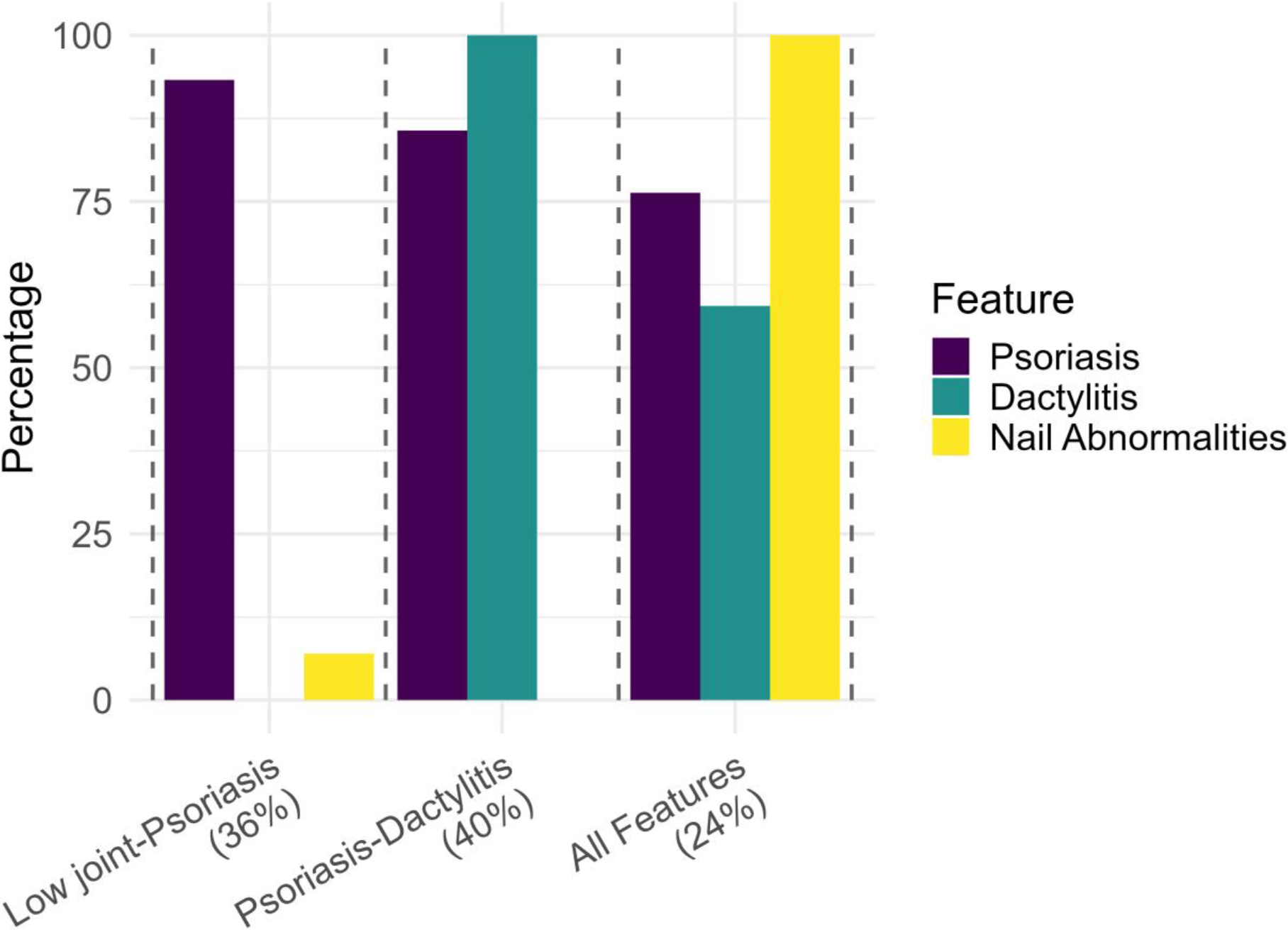
Results: In 3,282 children with a JPsA, ERA or uJIA diagnosis, symptom duration at first study documentation was median 11 months (IQR 3, 19). A total of 785 had a diagnosis of JPsA within two years of symptom onset, while 332 fulfilled ILAR criteria for JPsA, and 449 fulfilled CASPAR criteria for PsA. In the first 24 months following symptom onset, three JPsA clusters were consistently identified with significant differences across all outcomes (Figure 1): i) Low joint-Psoriasis , ii) Psoriasis-Dactylitis and iii) All Features . These groups made up 26%, 40% and 24% of those fulfilling ILAR criteria for JPsA, and 59%, 11% and 30% of those with a JPsA diagnosis, respectively. For those fulfilling CASPAR criteria for PsA, 53% and 42% were assigned to Psoriasis-Dactylitis and All Features groups. However, a third group differed: High joint-Dactylitis (5%). Several other disease and demographic features were associated with cluster assignment. Those in the Psoriasis-Dactylitis cluster tended to have the greatest disease burden. These children had the highest burden of enthesitis (70-83%, versus 19-21% All Features, 6-14%, Low joint-Psoriasis, 14% Only Dactylitis, p<0.001) alongside a greater proportion having a positive family history of psoriasis (57-85% versus 24-46% All Features, p<0.001). In addition, in those with a physician’s diagnosis of JPsA, the Psoriasis-Dactylitis cluster also experienced poorer patient/parent global scores (median 4.6, compared with 2.6-3.0, p=0.001), pain (median 5.1 compared with 3.0-3.5, p=0.003) and worse disability (median 1.0 compared with 0.3-0.4, p<0.001) compared with the other clusters. The Psoriasis-Dactylitis group tended to be younger than those in the All Features group (median 10-11yrs versus 12-13yrs, p<0.001) and were more likely to be female (65% versus 44%, p=0.007). In contrast, those in the Low joint-Psoriasis cluster had a lower disease burden, with significantly lower physician global scores (median 2.0-3.0cm versus 3.0-6.0cm) and ESR (median 10-12mm/hr versus 14-20mm/hr) compared with the Psoriasis-Dactylitis or All Features groups (all p<0.01). ANA was not associated with cluster assignment.
Conclusions: This large-scale international study demonstrates that JPsA is highly heterogenous, revealing distinct clusters with differing clinical features linked to inflammatory markers, family history and patient-reported outcomes. These patterns highlight meaningful biological variation and set the stage for future validation including an assessment of stability over time. They have the potential to inform both the earlier diagnosis and targeted treatment in children and young people with this disease.
REFERENCES: NIL.
Acknowledgments: NIL.
Disclosure of Interests: Stephanie Shoop-Worrall: None declared, Kimme Hyrich AbbVie, AbbVie, Sobi, Pfizer, BMS, Jaime Guzman: None declared, Kirsten Minden: None declared, Jens Klotsche: None declared, Roberta Berard: None declared, Rubén Queiro: None declared, Max Yates: None declared, Gerd-Marie Alenius: None declared, Flora McErlane: None declared, Coziana Ciurtin: None declared, Gavin Cleary: None declared, Laura C. Coates: None declared, Nophar Geifman: None declared.