fetching data ... 
Background: Mutations in the COL2A1 gene, which encodes the type II procollagen, cause a heterogeneous group of skeletal dysplasias by disrupting chondrocyte and vitreous matrix integrity. These mutations exhibit a wide clinical spectrum, ranging from articular degeneration to extraarticular dysfunction such as sensorineural hearing loss and ocular dysfunction. These disorders can clinically mimic inflammatory rheumatic diseases, such as rheumatoid arthritis (RA) or ankylosing spondylitis (AS). We present a case with a COL2A1 mutation misdiagnosed as seronegative RA and AS, leading to years of unnecessary immunosuppression.
Case Presentation: A 49 year old female patient presented to a rheumatology clinic in June 2018 due to progressive difficulty in walking, chronic hand and foot joint pain since the age of 15. Laboratory tests showed negative rheumatoid factor(RF) and anticyclic citrullinated peptide (anti-CCP), erythrocyte sedimentation rate:21 mm/h and CRP:5.3 mg/L. Based on these findings, the patient was diagnosed with seronegative RA and initiated on methotrexate.
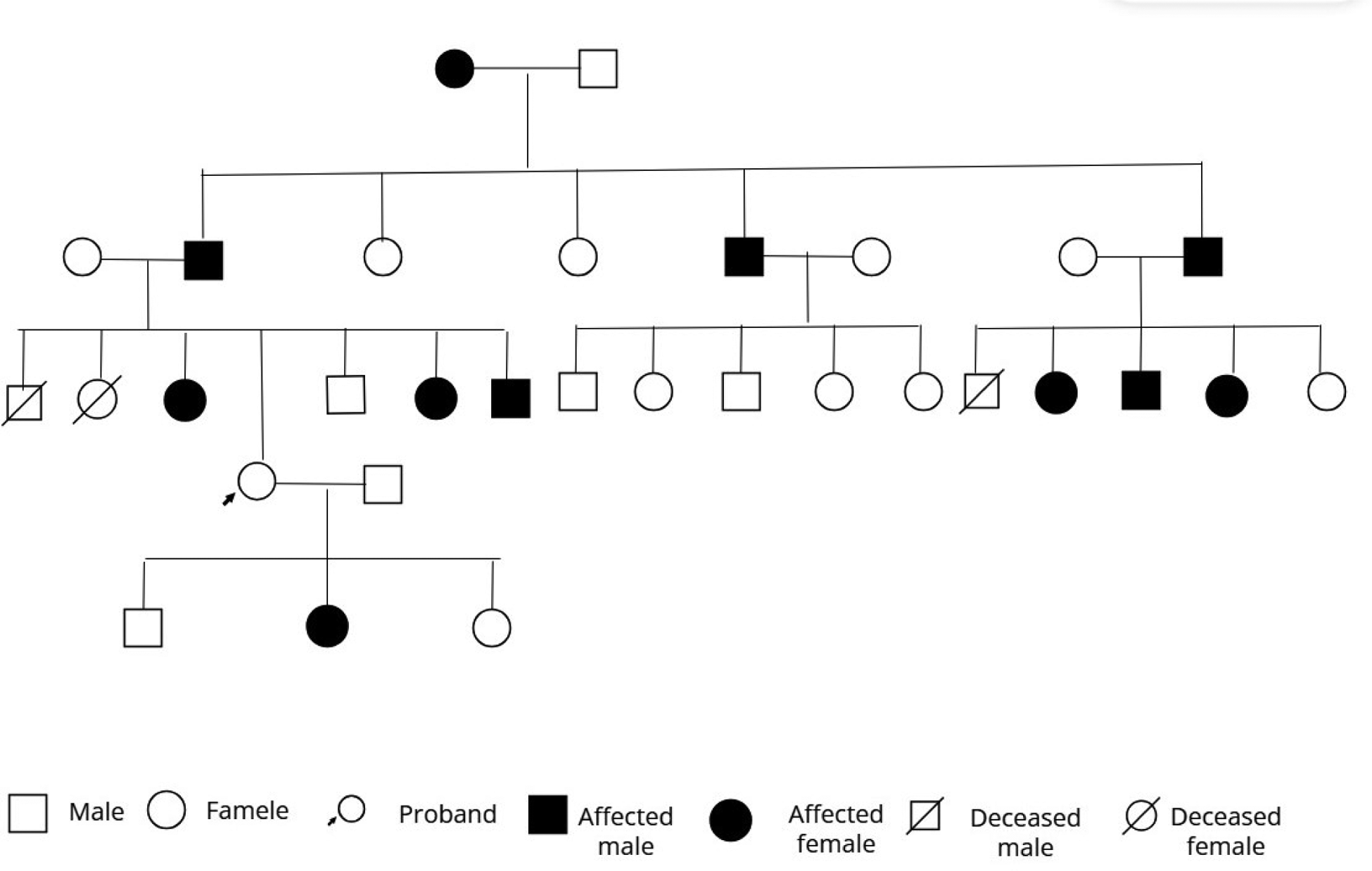
As no clinical improvement was observed follow-up, the treatment regimen was sequentially revised to methotrexate+sulfasalazine, followed by methotrexate+leflunomide+nonsteroidal antiinflammatory drugs(NSAIDs). In December 2020, following new-onset knee pain, the disease was considered active; etanercept was initiated. After two months of nonresponsiveness to etanercept, the patient was switched to adalimumab.The patient received two courses of adalimumab but discontinued treatment and follow-up. As low back and hip pain persisted, the patient was evaluated at another center with AS and was started on NSAIDs. Given partial improvement.The patient presented to our center in September 2024. Physical examination revealed significant kyphosis, flexion contractures of the knees. The FABER test was positive bilaterally and no signs of arthritis in other joints. RF, anti-CCP, human leukocyte antigen B27 were negative. Radiological imaging demonstrated bilateral grade 3 coxarthrosis, but sacroiliac joints were patent and spinal radiographs were inconsistent with spondylitis.In a patient with sensorineural hearing loss, family history revealed osteoarthritis and hearing loss in several relatives, including visual impairment in one. Due to the autosomal dominant inheritance pattern,the association of osteoarthritis with sensorineural hearing loss, a Type II Collagenopathy(COL2A1 related disease) was suspected. Genetic analysis identified the a pathogenic COL2A1 mutation. The patient was enrolled in rehabilitation and multidisciplinary follow-up was established alongside genetic counseling for the family.
Learning points for clinical practice: Misdiagnosed treatment-refractory seronegative arthritis harms patients and wastes resources; early COL2A1 genetic testing prevents unnecessary therapy, toxicity, disability and guides family care.
Results: Early genetic evaluation and detailed family history prevent misdiagnosis in treatment-refractory seronegative arthritis.
REFERENCES: NIL.
Acknowledgments: NIL.
Disclosure of Interests: None declared.