fetching data ... 
Background: Impaired physical function is common amongst people living with systemic lupus erythematosus (SLE), which can lead to significant impairments in quality of life, engagement with social and work activity, and increased healthcare costs. Functional decline in SLE is likely multifactorial, associated with not only higher disease activity and comorbidities but also non-disease-specific, psychosocial factors, such as depression and coping skills.
Objectives: To better understand these non-disease-specific drivers of perceived physical function in people with SLE, we aimed to investigate the associations of patient-reported psychosocial factors and fatigue with self-rated physical function in two demographically distinct SLE cohorts. In doing so, we sought to identify modifiable patient-reported factors that contribute to physical function, and inform more equitable and patient-centred approaches to assessment and management of SLE.
Methods: This cross-sectional study was conducted in two demographically distinct, population-based cohorts of adults (≥18) with a clinician-confirmed diagnosis of SLE: Approaches to Positive, Patient-centered Experiences of Aging with Lupus (APPEAL), recruited from the Georgians Organized Against Lupus cohort; and the California Lupus Epidemiology Study (CLUES). The outcome of perceived physical function was assessed using PROMIS Physical Function-Short Forms 12a (APPEAL) and 10a (CLUES). For both instruments, raw scores were scaled to comparable T-scores, in which 50 represents the average score amongst adults in the general population, 1 SD is represented by differences of 10, and higher scores denote better perceived physical function. Exposures were assessed via validated questionnaires, as follows: i) fatigue, using a single item from the Systemic Lupus Erythematosus Questionnaire (SLAQ); ii) depression, using the 8-item PROMIS depression scale T-scores (APPEAL) and Patient Health Questionnaire-8 question (PHQ-8; CLUES); iii) stress, using the 10-item Perceived Stress Scale (PSS-10; APPEAL) and 4-item PSS (PSS-4; CLUES); iv) coping efficacy (Coping Self-Efficacy Scale) and learned helplessness (Rheumatology Attitudes Index) (APPEAL only); v) resilience (Brief Resilience Coping Scale) and self-efficacy (PROMIS General Self-Efficacy 4a) (CLUES only). PROMIS scores were presented as T-scores; PSS, coping resilience and learned helplessness measures were z-standardised to facilitate direct comparisons between cohorts. Multivariable linear regression analyses were conducted to assess the association of patient-reported outcomes with physical function psychosocial, adjusting for age, sex, and race.
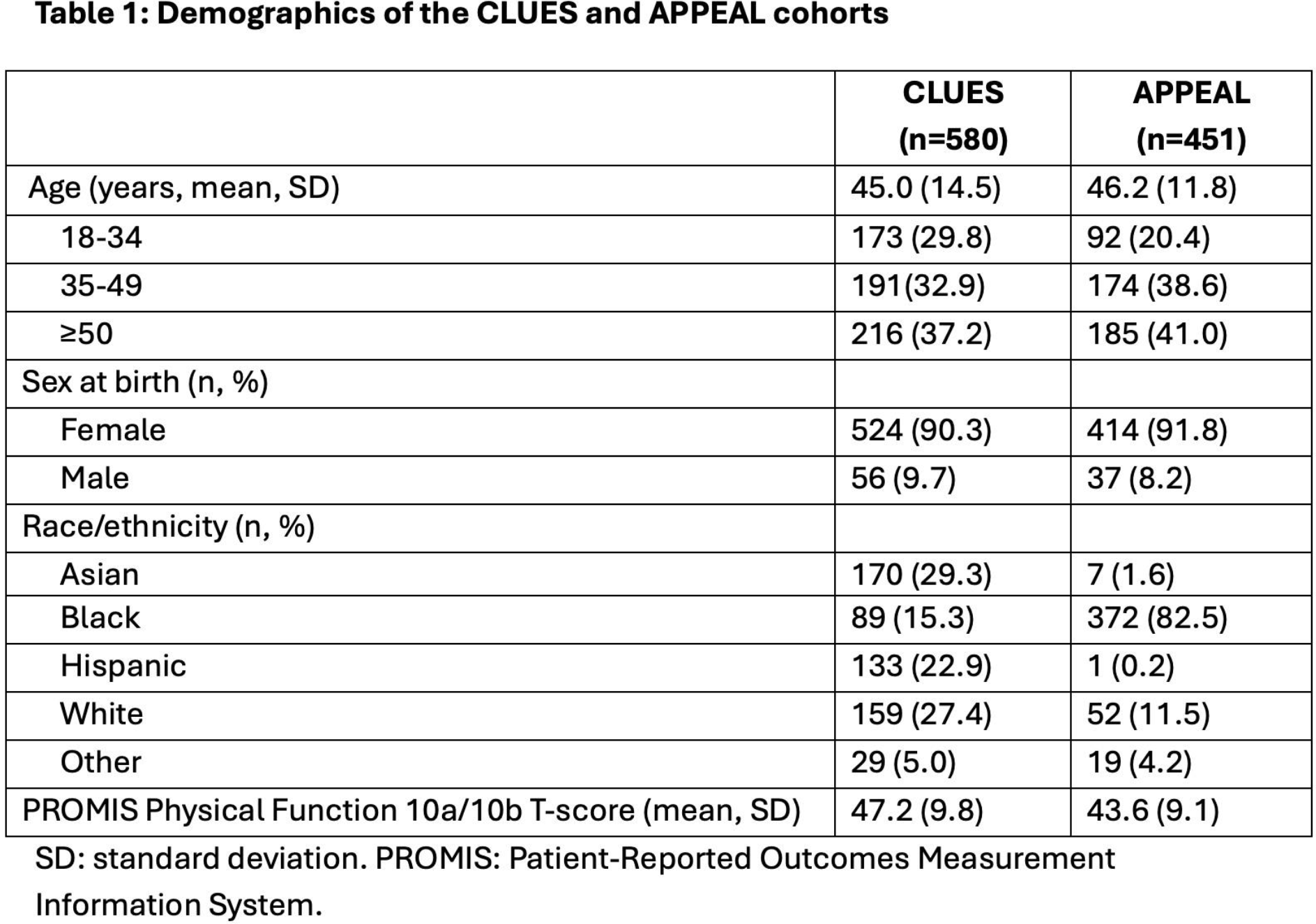
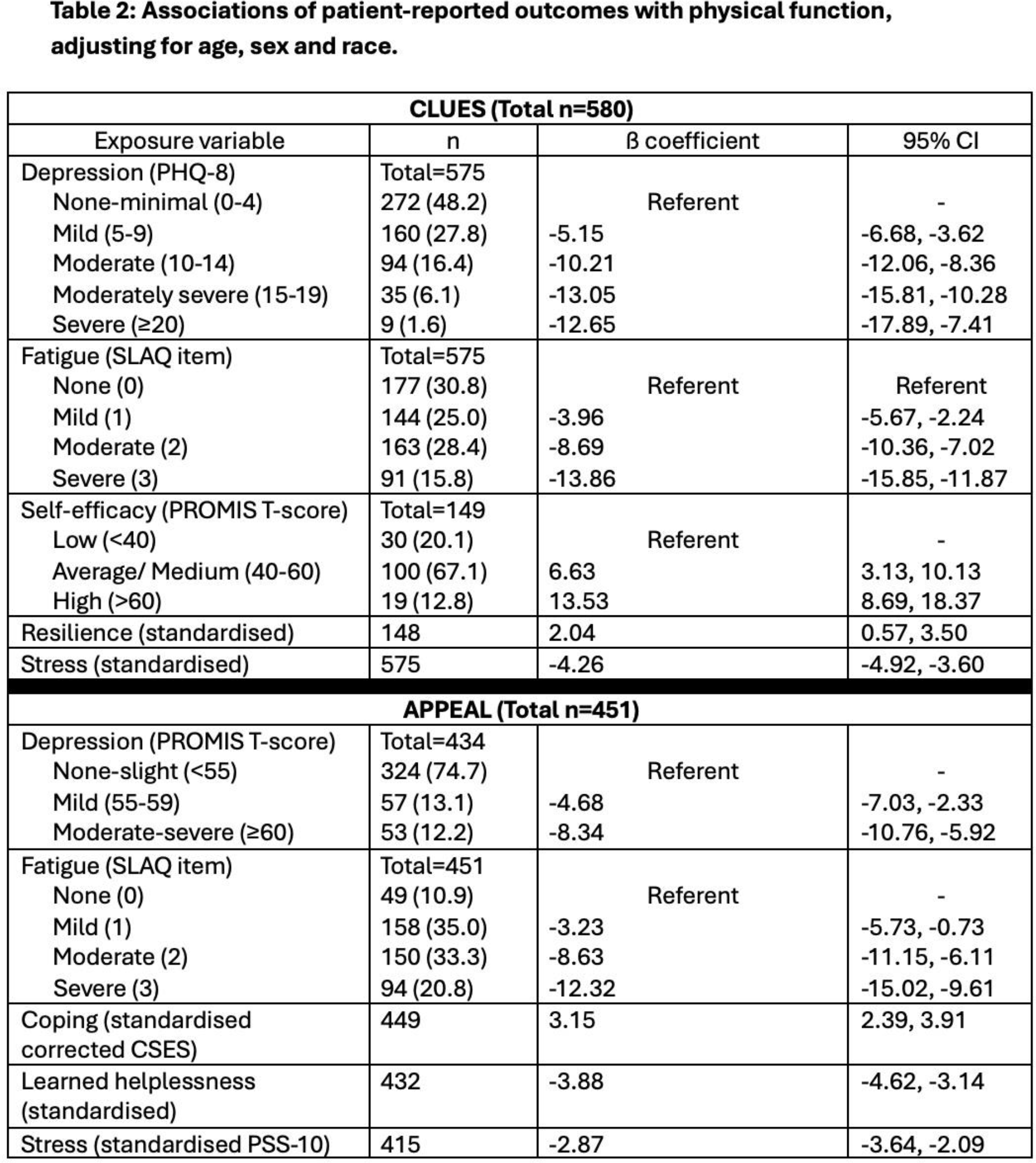
Results: APPEAL participants (N=451) were primarily Black (82.5%); CLUES participants (N=580) were predominantly Asian (29.3%), Hispanic (22.9%), and White (27.4%) (Table 1). Age and sex were comparable between cohorts. However, APPEAL had a slightly higher proportion of older individuals compared to CLUES, with 41.0% vs 37.2% being ≥50 years. Mean perceived physical function T-scores were lower in APPEAL (43.6) compared to CLUES (47.2; P<0.05). The most severe levels of fatigue were reported by 15.8% vs. 20.8% of participants in CLUES vs. APPEAL, respectively. In both cohorts, greater fatigue was statistically significantly associated with worse physical function. A greater strength of association observed at all three categories of fatigue in CLUES vs APPEAL (Mild: ß -3.96 [95% CI -5.67, -2.24] vs ß -3.23 [-5.73, -0.73]; Moderate: ß -8.69 [-10.36, -7.02] vs ß -8.63 [-11.15, -6.11]; Severe: ß -13.86 [-15.85, -11.87] vs ß -12.32 [-15.02, -9.61]) (Table 2). With regards to depression, a greater proportion of participants reported moderate-severe levels in CLUES (24.1%), compared to APPEAL (12.2%). In both cohorts, worse depression, i.e. moderate-severe vs mild-none, was associated with >1 SD lower physical function score. A greater strength of association was observed in CLUES vs APPEAL, especially at higher levels of depression: CLUES, Moderately severe: ß -13.05 (-15.81, -10.28); Severe: ß -12.65 (-17.89, -7.41); APPEAL, Moderate-severe: ß -8.34 (-10.76, -5.92). Mean PSS-4 score in CLUES was 5.0 (SD 3.3, range 0-16); mean PSS-10 score in APPEAL was 15.2 (SD 7.1, range 0-40). Z-standardised scores in both datasets were close to zero. In both cohorts, worse perceived stress was significantly associated with worse physical function, although the magnitude of association was greater in CLUES (ß -4.26 [95% CI -4.92, -3.60]) compared to APPEAL (ß -2.87 [95% CI -3.64, -2.09]). Greater resilience (per +1 SD: ß=2.04 [0.57, 3.50]) and self-efficacy (high [PROMIS T-score >60] vs. low (T-score <40): ß =13.53 [8.69, 18.37]; both in CLUES), and better coping (per +1 SD: ß =3.15 [2.39, 3.91]; in APPEAL) were associated with better physical function. In APPEAL, greater learned helplessness was associated with worse physical function (per +1SD: ß =-3.88 [-4.62, -3.14]).
Conclusions: In this study of two socio-demographically distinct cohorts of people with SLE, we found that patient-reported factors, including fatigue, depression, stress, coping, and self-efficacy, were consistently and strongly associated with perceived physical function. Despite marked differences in cohort composition, similar patterns of association were observed in both populations, highlighting an important relationship between psychosocial and subjective experiences and perceived physical function in SLE. To our knowledge, this is the first and largest study to demonstrate such findings in distinct and diverse cohorts of individuals with SLE. Our findings reinforce the importance of routinely incorporating patient-reported outcomes into clinical practice, not only to capture patient experiences but also to inform prognostic assessment and guide holistic, patient-centred care.
REFERENCES: NIL.
Acknowledgments: NIL.
Disclosure of Interests: None declared.