fetching data ... 
Background: Digital patient education shows promise in supporting self-management in rheumatoid arthritis (RA) [1]. However, variation in patients’ health literacy and e-health literacy may influence engagement with digital health interventions [2, 3], potentially excluding individuals with limited health literacy or digital skills. Therefore, consideration of patients’ health literacy and e-health literacy competencies is important when developing and implementing digital health interventions to accommodate diverse patient needs and ensure accessibility and fit-for-purpose solutions.
Objectives: This study aimed to investigate e-health literacy levels and identify e-health literacy profiles in a Danish RA cohort, to inform the development of tailored patient education pathways, specifically to improve access to an existing digital patient education intervention while accommodating varying support needs and e-health literacy diversity.
Methods: Elements of the Optimizing Health Literacy and Access (Ophelia) process (a structured method to enhance health literacy and improve healthcare access) were applied [4]. e-health literacy strengths, challenges, and needs were assessed via a survey using the eHealth Literacy Questionnaire (eHLQ) [5], supplemented with data on demographics, quality of life, physical function, and comorbidities. The survey was distributed electronically via e-Boks, the national secure digital mailbox mandatory for Danish citizens aged 15 and older. To enhance representation of individuals with limited digital access, patients exempt from e-Boks were invited by postal mail and could respond either on paper or via a telephone interview. Cluster analysis identified subgroups with similar eHLQ patterns, forming patient profiles. Next, vignettes portraying fictional persons typical of each patient profile were developed using survey data, qualitative interviews with patients, and clinical experience from the research group. This was followed by a co-design process involving workshops with patients and health professionals. Using the developed vignettes as a starting point for discussion, the workshops explored patients’ e-health literacy related needs, potential challenges, and health service responsiveness. The aim was to identify potential actions to tailor patient education pathways, including both digital and alternative non-digital approaches, to support self-management and engagement in RA care. Finally, a prioritisation workshop involving members of the research group and a patient research partner, followed by discussions with clinical leaders and nurses, determined which actions to implement in practice.
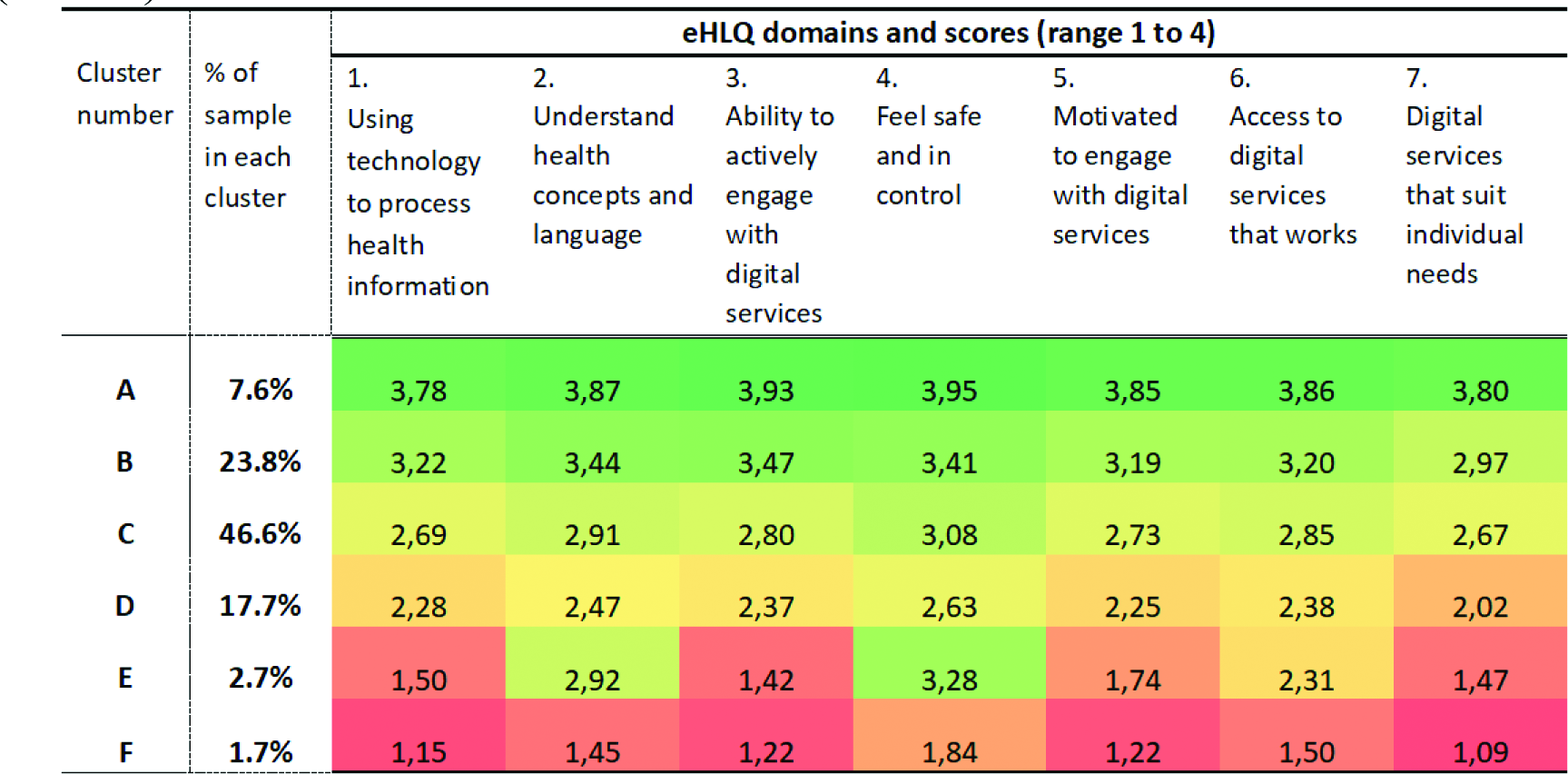
Results: Data from 661 patients were included in the cluster analysis, revealing six profiles with distinct e-health literacy strengths and challenges (Figure 1). Participants had a median age of 66 years (IQR 56 to 73), 69.6% were female, and median disease duration was 12.5 years (IQR 6 to 23). Most lived with another adult (66.9%), and 48.4% had an educational level corresponding to medium-cycle, bachelor’s, or long-cycle higher education. Employment status and household income varied. The majority (78%, Profiles A–C) showed moderate to high e-health literacy scores and potential to engage with digital patient education. Profiles A and B were likely able to use digital patient education independently, while Profile C might need some support and assistance. The remaining 22% (Profiles D–F) faced multidimensional barriers, particularly Profiles E and F, indicating a need for significant guidance to benefit from digital patient education, or the provision of non-digital alternatives.
Six vignettes representing the patient profiles were developed. Co-design workshops with eight patients and four health professionals generated 29 key considerations to enhance engagement with digital patient education or alternative educational support, including 13 identified by patients and 16 by health professionals. There was considerable thematic overlap between patient and professional ideas, and five of the professional ideas had previously been identified by rheumatology nurses. Following prioritisation and merging of duplicate concepts, 13 major action ideas were selected. Examples of the prioritised action ideas included assisting patients with app setup, highlighting benefits of digital patient education, offering non-digital alternatives (face-to-face education, written materials), sharing the app with relatives, postcards/materials to inform about the app, reducing response time for chat messages in the app, and screening for digital literacy.
Conclusions: Diverse e-health literacy profiles highlight the need for differentiated patient education approaches. While many patients can engage with digital patient education independently or with limited support or assistance, approximately one-fifth require tailored alternatives. Hence, an e-health literacy-informed, differentiated approach can support engagement in digital patient education and promote inclusive implementation.
Heat map showing the 6 clusters identified through the cluster analysis of eHLQ data (N=661)
REFERENCES: [1] Knudsen LR, et al. Rheumatology (Oxford). 2024;63(9):2547-56.
[2] Bakker MM, et al. Arthritis Care Res (Hoboken). 2021;73(1):100-9.
[3] Hider S, et al. Rheumatol Adv Pract. 2023;7(1):rkac109.
[4] Osborne RE, et al. Centre for Global Health and Equity, Swinburne University of Technology, Melbourne, Australia. 2021.
[5] Kayser L, et al. J Med Internet Res. 2018;20(2):e36.
Acknowledgments: NIL.
Disclosure of Interests: Line Raunsbæk Knudsen LEO Pharma, Sofie Bech Vestergaard: None declared, Mark Matthijs Bakker: None declared, Mwidimi Ndosi: None declared, Annette de Thurah: None declared.