fetching data ... 
Background: Rheumatoid arthritis (RA) predominantly affects women. The menopausal transition represents a critical hormonal shift that may modify inflammatory burden. While younger women with RA have been extensively studied, postmenopausal women remain underrepresented in clinical research, particularly regarding their response to biologic DMARDs (bDMARDs). Clarifying the impact of menopause on RA presentation and therapeutic response is essential to optimize personalized treatment strategies in women across different reproductive stages.
Objectives: To investigate clinical and treatment-related differences between women with RA of childbearing age and postmenopausal women initiating a bDMARD, and to assess whether menopausal status influences treatment effectiveness. A secondary objective was to identify predictors of early remission among postmenopausal women and to explore the impact of RA onset before versus after menopause on treatment outcomes.
Methods: Female RA patients starting bDMARD between January 2016 and December 2025 were included in this multicentre real-world observational study based on the Italian “BIOlogic aPUlian Registry” (BIOPURE). Demographic, laboratory, imaging and clinical data (including childbearing and menopausal status) were collected at baseline and at four-months interval thereafter. Data were analysed at 6 (T6), 12 (T12) and 24 (T24) months of follow-up. Patient characteristics were compared between childbearing age (Cb/fRA) and postmenopausal (PMp/fRA) women using Mann-Whitney test or Chi-square test as appropriate. Logistic regression was used to investigate the association between selected variables and DAS28-CRP remission achievement at T6, reporting as adjusted odds ratio (adjOR) with 95% confidence interval (CI), adjusting for confounders as DAS28-CRP value, seropositivy status and steroid user at baseline.
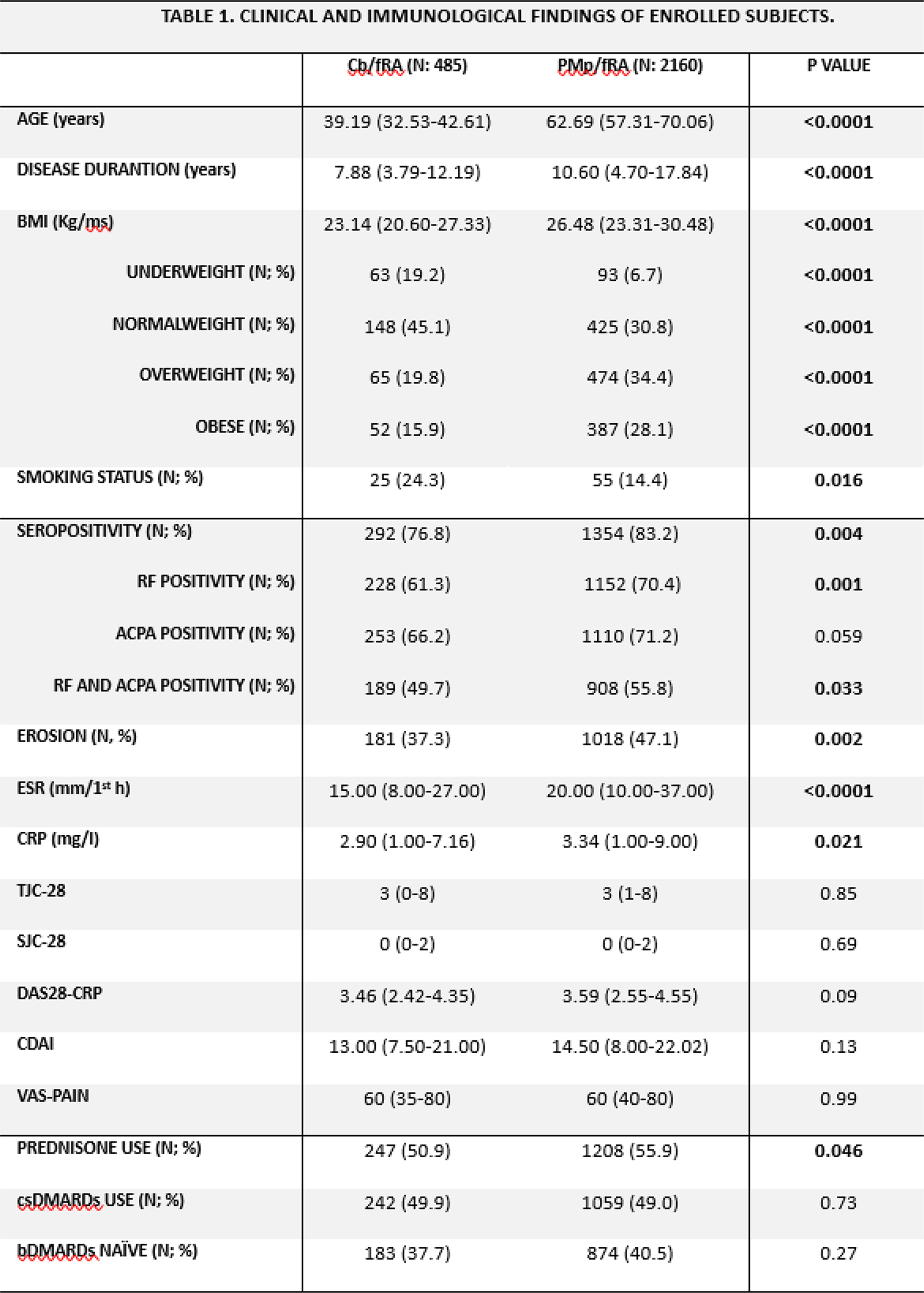
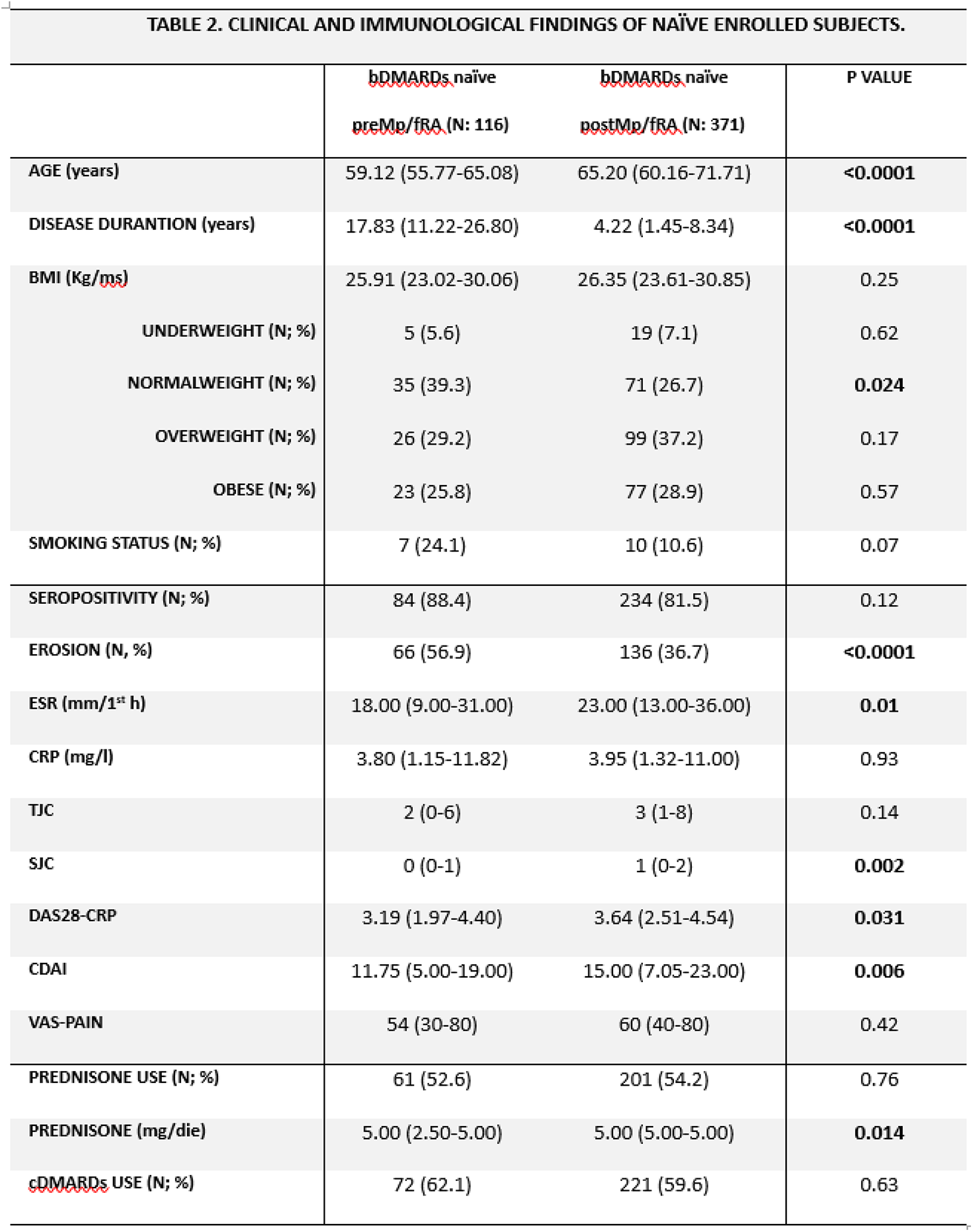
Results: A total of 2645 consecutive female RA patients were enrolled, comprising 485 Cb/fRA and 2160 PMp/fRA (tab.1). At baseline, PMp/fRA showed a more severe disease phenotype compared to Cb/fRA in terms of RF or ACPA positivity (83.2% vs 76.8% respectively, p= 0.004), being more erosive (47.1% vs 37.3% respectively, p= 0.002) and characterized by higher CRP level (3.34 vs 2.90 mg/l respectively, p= 0.021), with a higher prevalence of glucocorticoid use (55.9% vs 50.9%,respectively, p= 0.046). Despite these differences, disease activity at baseline was comparable between groups, with similar DAS28-CRP (p= 0.09) and CDAI values (p= 0.13). During follow-up, PMp/Fra maintained a higher rate of glucocorticoid use (T12: 49.46%; T24: 18.42%) compared to Cb/fRA (T12: 18.42%, p< 0.0001; T24: 10.71%, p< 0.0001). Achievement of DAS28-CRP remission was significantly more frequent in Cb/fRA compared to PMp/fRA (64.9% vs 53.6%, p< 0.0001). Considering PMp/Fra, early remission at T6 was more likely in patients who were in Rem/LDA (OR= 4.526 (3.492-5.865)), bDMARD-naïve (OR= 1.694 (1.354-2.119)) and not affecting by fibromyalgia (OR= 1.875 (1.249-2.814)). In multivariable analysis, these features predicted DAS28-CRP remission at T6 (adjOR= 2.004 (1.017-3.947))). No differences in remission rates were observed according to the mechanism of action of the bDMARD treatment. Among PMp/fRA, those with RA onset before menopause (preMp/fRA) higher rates of seropositivity (87.2%) and erosive (66.4%) disease compared with those with postmenopausal-onset RA (postMp/fRA) (80.0%, p= 0.002 and 42.1%, p< 0.0001). Restricting the analysis to bDMARD-naïve patients, women with premenopausal-onset RA were more erosive (56.7%) but less disease activity (DAS28-CRP: 3.19; CDAI: 11.75) at treatment initiation compared to postmenopausal-onset patients (erosion: 36.7%, p< 0.0001; DAS28-CRP: 3.64, p= 0.031; CDAI: 15.00, p= 0.006). Notably, despite these distinct disease trajectories, DAS28-CRP remission rates at different timepoints were comparable between groups (tab.2).
Conclusions: Menopausal status identifies distinct RA phenotypes at the time of bDMARD initiation. Postmenopausal women RA patients present with a more severe immune and radiological profile and a lower likelihood of achieving remission compared with women of childbearing age, despite similar baseline disease activity. However, early remission remains achievable in postmenopausal patients, particularly among those who are bDMARD-naïve, are not affecting by fibromyalgia and with lower inflammatory burden, independently of the biologic mechanism of action. Furthermore, RA onset before or after menopause defines different pathways to bDMARD initiation (radiographic progression in preMp/fRA versus inflammatory activity in postMp/fRA) without ultimately affecting short-term treatment effectiveness. These findings support the need for tailored therapeutic strategies in postmenopausal women with RA and highlight early disease control as a critical determinant of treatment success in this population.
Cb/fRA: female RA patients of childbearing age; PMp/fRA: postmenopausal female RA patients; BMI: Body Mass Index; Kg/ms: kilogram per metre squared; RF: Rheumatoid Factor; ACPA: Anti-Citrullinated Protein Antibody; ESR: erythrocyte sedimentation rate; CRP: C-reactive protein; TJC-28: tender joint count; SJC-28: swollen joint count; VAS-PAIN: pain visual analog scale. Median and interquartile range or frequency and percentages are shown as appropriated. P-value ≤0.05 was considered statistically significant.
preMp/fRA: female RA patients with RA onset before menopause; postMp/fRA: female RA patients with RA onset after menopause; BMI: Body Mass Index; Kg/ms: kilogram per metre squared; RF: Rheumatoid Factor; ACPA: Anti-Citrullinated Protein Antibody; ESR: erythrocyte sedimentation rate; CRP: C-reactive protein; TJC-28: tender joint count; SJC-28: swollen joint count; VAS-PAIN: pain visual analog scale. Median and interquartile range or frequency and percentages are shown as appropriated. P-value ≤0.05 was considered statistically significant.
REFERENCES: NIL.
Acknowledgments: NIL.
Disclosure of Interests: None declared.