fetching data ... 
Background: Perimenopause is associated with a wide spectrum of symptoms, including mood changes, sleep disturbances, and joint pains. Limited information exists on the effect of perimenopause in psoriatic arthritis (PsA).
Objectives: We aimed to assess whether PsA disease activity worsens during perimenopause compared to pre- and post- menopause stage among patients with PsA followed prospectively.
Methods: We analyzed data on female patients with PsA followed in a prospective cohort from 1978 to 2024. Data on PsA disease activity, medications, co-morbidities, and age at menopause were collected using standard protocols. Pre-perimenopause and post-menopause stages were defined as >2 years before and after the final menstrual period (FMP), respectively, while the perimenopause stage was within 2 years (before or after) of the FMP. PsA disease activity was assessed at each visit using Disease Activity in PsA (DAPSA), tender joint count (TJC) and swollen joint count (SJC), PASI, CRP, and FACIT-fatigue. Disease activity during the perimenopause stage was compared to the pre-perimenopause and post-menopause visits. The association between menopausal stages and PsA disease activity measures was assessed with a Generalized Additive Model with splines (considering time from FMP as continuous) and with linear mixed-effects models (considering menopausal stages as categorical variables). Each model was adjusted for age, disease duration, and medication use, and accounted for repeated observations via a subject-specific random effect. We assessed the mediating effects of BMI and fatigue on the change in DAPSA across menopause stages.
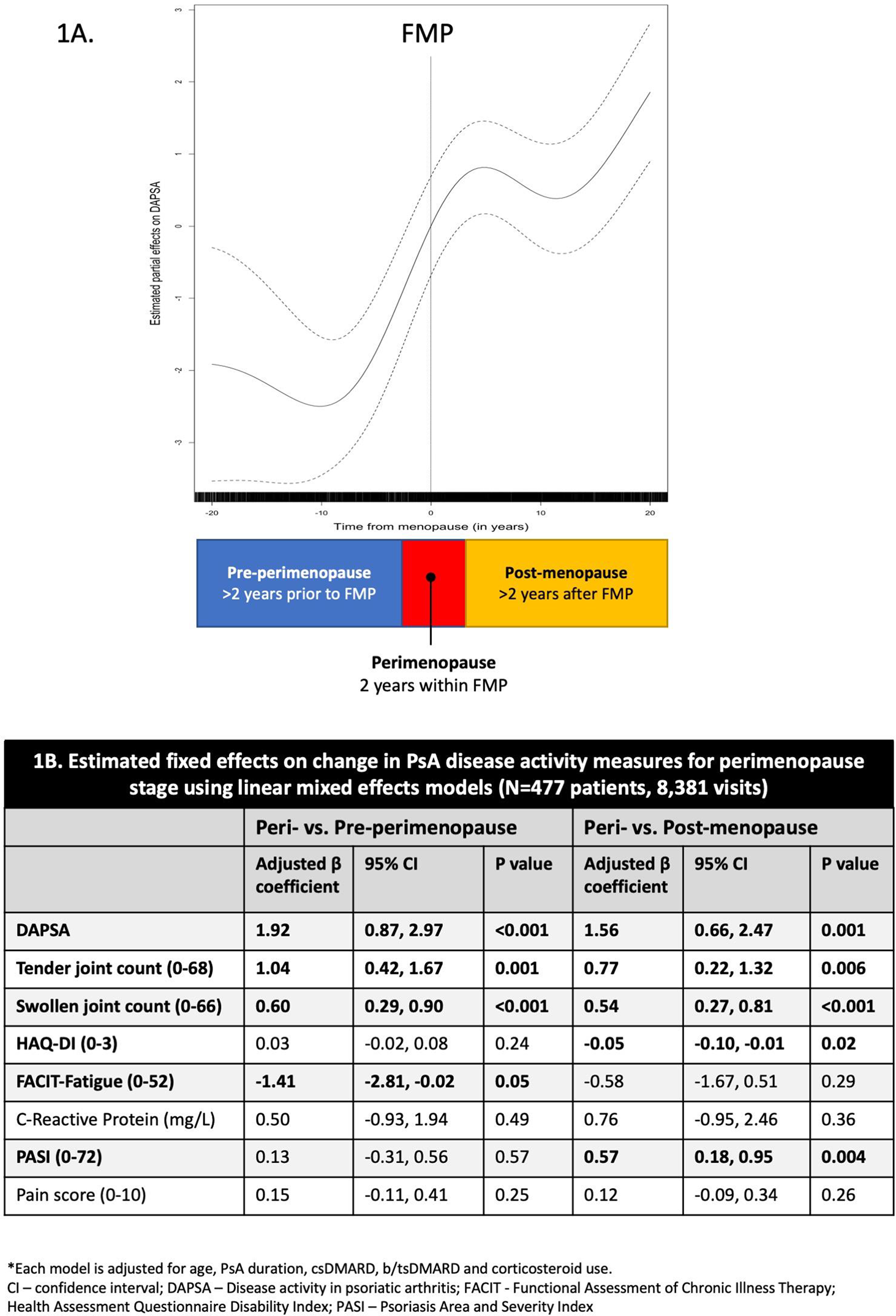
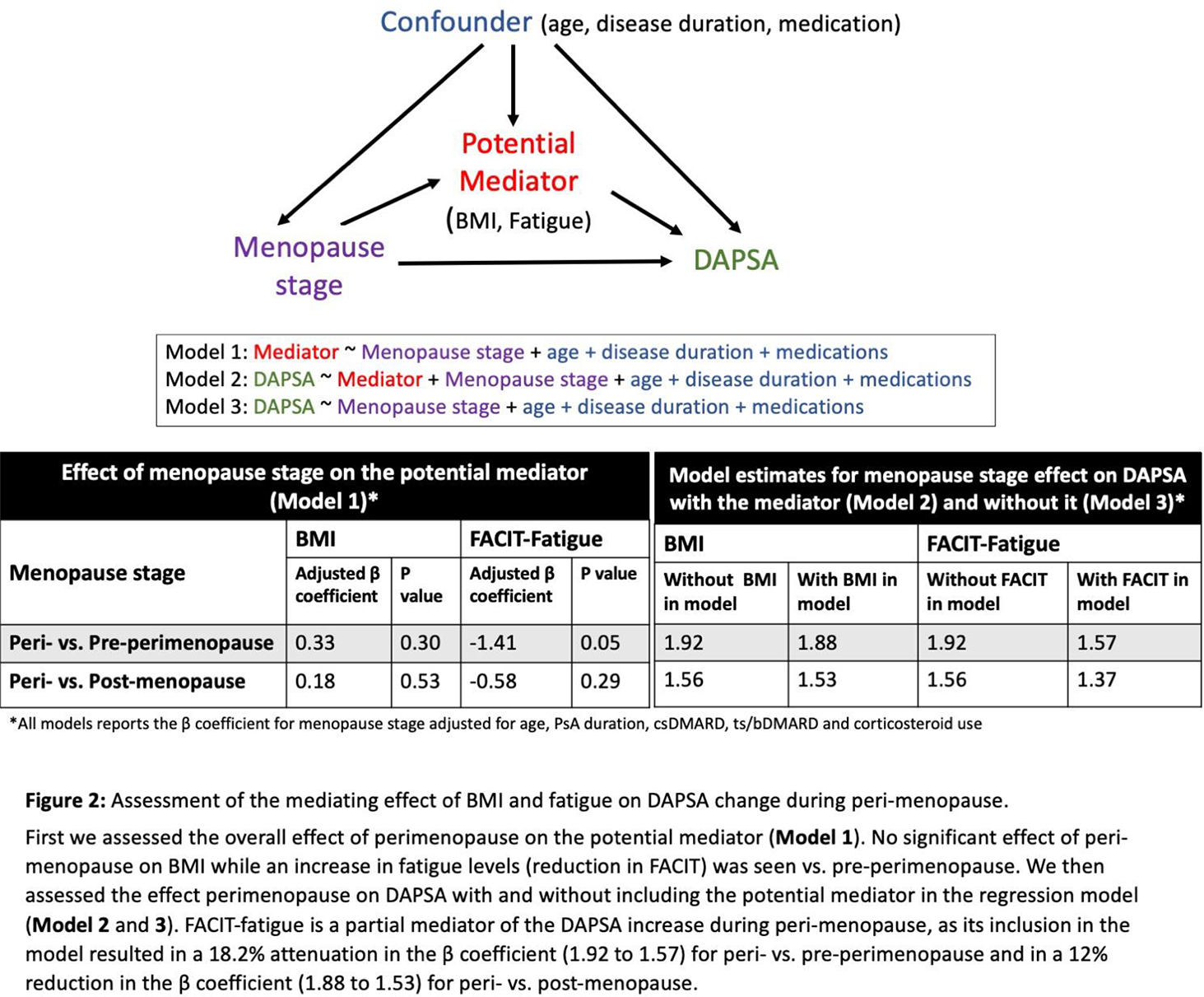
Results: A total of 477 female patients provided data for 8,381 visits over a mean follow-up of 12.1 years. Mean age at first visit was 44.9±13.9 years and mean age at menopause was 48.7 years. Hormone replacement therapy had only been used during 1.5% of visits. A rise in DAPSA scores was found during perimenopause years, followed by a slight drop post menopause (Figure 1A). Linear mixed models found an association between being in perimenopause and higher DAPSA vs. pre-perimenopause (β 1.92, 95% CI 0.87, 2.97; p<0.001) and post-menopause stages (β 1.56, 95% CI 0.66, 2.47; p=0.001, Figure 1B). Significantly higher TJC and SJC were found in perimenopause vs. both pre- and post-menopause (TJC peri- vs. pre: β 1.04, 95% CI 0.42, 1.67; peri- vs. post: β 0.77, 95% CI 0.22, 1.32; and SJC peri- vs. pre: β 0.60, 95% CI 0.29, 0.90; peri- vs. post: β 0.54, 95% CI 0.27, 0.81). Higher PASI was found in perimenopause vs. post-menopause stage (Figure 1B). Increase in fatigue levels during perimenopause only partially mediated the increase in DAPSA score during perimenopause, explaining 12% to 18% of this change (Figure 2). BMI did not have a mediating effect on DAPSA change during perimenopause.
Conclusions: Perimenopause is associated with an increase in PsA disease activity which includes both patient-reported outcomes but also objective measures of activity. These findings may warrant consideration of hormone replacement therapy in perimenopausal PsA patients.
A: Time from final menstrual period (FMP) estimated partial effect on the individual mean DAPSA score by Generalized Additive Model adjusted for age, disease duration and medication use; 1B: The estimated fixed effects on change in PsA disease activity measures for perimenopause stage using linear mixed effects models.
Assessment of the mediating effect of BMI and fatigue on DAPSA change during peri-menopause.
REFERENCES: NIL.
Acknowledgments: NIL.
Disclosure of Interests: Lihi Eder Abbvie, J&J, Eli Lilly, BMS, UCB, Pfizer, Moonlake, Novartis, Abbvie, Eli Lilly, J&J, Pfizer, Novartis, BMS, UCB, Fresenius Kabi, Xianwei Li: None declared, Sahil Koppikar AbbVie, Eli Lilly, Fresenius Kabi, JAMP, J&J, Novartis, Pfizer, Sandoz, UCB, AbbVie, Pfizer, Novartis, Illiana Lega: None declared, Dafna Gladman Abbvie, Amgen, BMS, Eli Lilly, Fresenius Kabi, Johnson and Johnson, Novartis, Pfizer and UCB, Abbvie, Amgen, BMS, Eli Lilly, Fresenius Kabi, Johnson and Johnson, Novartis, Pfizer and UCB, Vinod Chandran Spouse is employed by AstraZeneca, AbbVie, BMS, Eli Lilly, Fresenius Kabi, Janssen, Novartis, UCB. Leadership role or fiduciary role in other board: Group for Assessment of Psoriasis and Psoriatic Arthritis., AbbVie/Abbott, Richard Cook: None declared.