fetching data ... 
Background: Autoantibody internalization has been implicated in the pathogenesis of autoimmune diseases, yet its underlying mechanisms and generality across diseases, cell types, and affected tissues remain poorly understood.
Objectives: To define the mechanism of autoantibody internalization and assess its generality across different autoimmune diseases, cell types, and tissues.
Methods: Bulk RNA sequencing was performed on 815 diagnostic muscle biopsies spanning autoantibody-defined myopathies and related systemic autoimmune diseases, with validation in an independent anti-PM/Scl cohort (n=41). Transcriptomic analysis was also performed on cultured human muscle cells following the introduction of purified patient immunoglobulin by electroporation. Direct immunofluorescence was used to localize IgG in muscle and skin. Spatial transcriptomics mapped disease-specific transcripts, immunoglobulin transcripts, cell-type markers, and interferon modules to define spatial relationships among intracellular effects, tissue damage, inflammation, and local antibody sources.
Results: Bulk RNA sequencing identified reproducible, autoantibody-specific transcriptomic signatures consistent with autoantigen dysfunction in muscle biopsies from patients with anti-Mi2 + dermatomyositis and anti-PM/Scl + scleromyositis across independent cohorts. Electroporation of purified patient IgG into primary cultures of healthy cells was sufficient to induce the corresponding disease-specific transcriptomic programs in vitro. Direct immunofluorescence demonstrated immunoglobulin internalization into subcellular compartments corresponding to autoantigen localization in muscle and skin. Spatial transcriptomic analyses revealed that plasma cells released cytoplasmic material, including immunoglobulin RNA, into adjacent affected cells expressing autoantibody-specific transcripts (Figures 1 and 2). Disease-specific transcripts were detected not only in muscle fibers (Figures 1 and 2) but also in other cell types, including endothelial cells and fibroblasts. These changes were associated with cellular damage and autoantibody-specific inflammatory responses, including activation of type I interferon signaling in anti-Mi2 + dermatomyositis and type II interferon signaling in anti-PM/Scl scleromyositis (Figures 1 and 2). Autoantibody internalization was also observed in muscle and skin from patients with other autoimmune diseases, including anti-U1RNP mixed connective tissue disease, anti-Ku overlap syndrome, and anti-Scl70 systemic sclerosis.
Conclusions: These findings establish autoantibody internalization as a shared pathogenic mechanism across diverse autoimmune diseases, providing a unifying framework for conditions driven by autoantibodies targeting intracellular antigens.
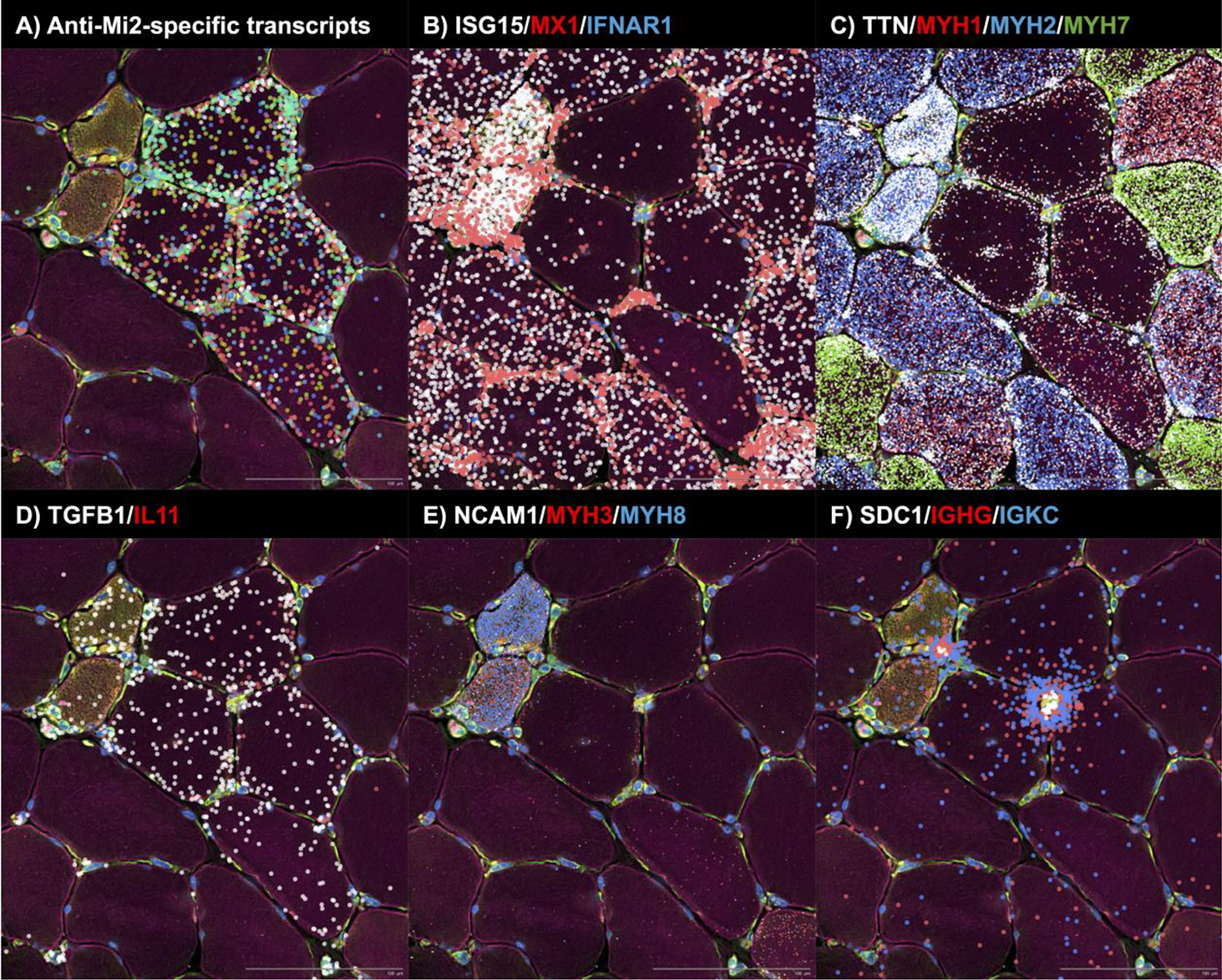
. Spatial transcriptomic analysis of a representative biopsy area from an anti-Mi2–positive patient, highlighting molecular signatures consistent with autoantibody internalization, autoantibody internalization–associated tissue damage, and the transfer of immunoglobulin transcripts from plasma cells to adjacent muscle cells. Colored dots indicate the spatial distribution of: (A) anti-Mi2–specific transcripts; (B) type I interferon–inducible genes (ISG15, MX1) and the interferon receptor IFNAR1; (C) transcripts associated with mature muscle fibers (TTN) and specific muscle fiber types (MYH1, type IIx; MYH2, type IIa; MYH7, type I); (D) TGFB1 and IL11; (E) markers of muscle regeneration (NCAM1, MYH3, MYH8); and (F) plasma cell markers (SDC1), immunoglobulin G heavy-chain constant region (IGHG), and immunoglobulin kappa constant region (IGK).z
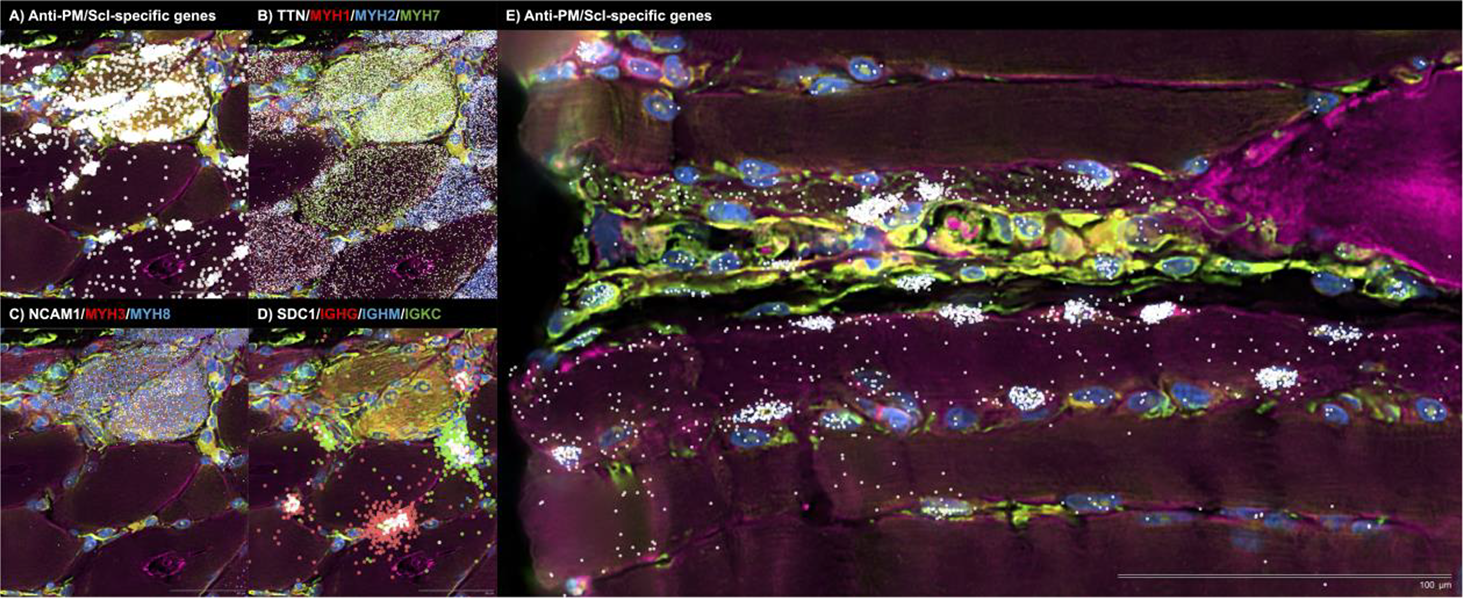
. Spatial transcriptomic analysis of two representative biopsy regions from an anti–PM/Scl–positive patient, highlighting molecular signatures consistent with autoantibody internalization, autoantibody internalization–associated tissue damage and the transfer of immunoglobulin transcripts from plasma cells to adjacent muscle cells. In both panels, colored dots depict the spatial distribution of: (A, E) anti–PM/Scl–specific transcripts; (B) transcripts associated with mature muscle fibers (TTN) and specific fiber types (MYH1, type IIx; MYH2, type IIa; MYH7, type I); (C) markers of muscle regeneration (NCAM1, MYH3, MYH8); and (D) plasma cell markers (SDC1), immunoglobulin G heavy-chain constant region (IGHG), immunoglobulin M heavy-chain constant region (IGHM), and immunoglobulin kappa constant region (IGKC).
REFERENCES: NIL.
Acknowledgments: NIL.
Disclosure of Interests: None declared.