fetching data ... 
Background: While CD19 CAR-T therapy offers the potential for sustained drug-free remission in refractory autoimmune diseases, maintaining this remission remains challenging for some patients. To elucidate the durability of remission and enable early detection of relapse, biomarkers that longitudinally monitor immune reset are required. Serial serum proteomics enables quantification of post-treatment immune dynamics and characterisation of distinct immune trajectories.
Objectives: This study aims to characterise longitudinal serum proteomic changes after CD19 CAR-T therapy in patients with durable remission (DR) and examine differences in these patterns between patients who maintain DR and those who relapse.
Methods: We tracked serum proteomic profiles over time in patients with systemic lupus erythematosus (SLE), systemic sclerosis (SSc), and Idiopathic Inflammatory Myopathies (IIM) who underwent CD19 CAR-T therapy, using the NULISAseq™ Inflammation Panel 250. The study included 25 participants (11 with SLE, 10 with SSc, and 4 with IIM), from whom 150 serum samples were collected, spanning from the pre-infusion period (day −46 to 0) to follow-up (up to day 994). Durable remission (DR) was defined as remaining relapse-free for at least 800 days; patients with shorter follow-up who had not relapsed were excluded from the comparison. To identify proteins with time-dependent changes in the DR group, protein abundance was modelled using linear regression with natural cubic splines for time, accounting for within-subject correlation and disease effects, followed by empirical Bayes moderation. Proteins with a significant change over time in DR patients were clustered into five distinct modules (c1–c5) based on their trajectories from baseline, and module scores were calculated using GSVA. The longitudinal trajectories of these modules were assessed in the DR and relapse subjects using a similar model, followed by F-tests with false discovery rate (FDR) correction.
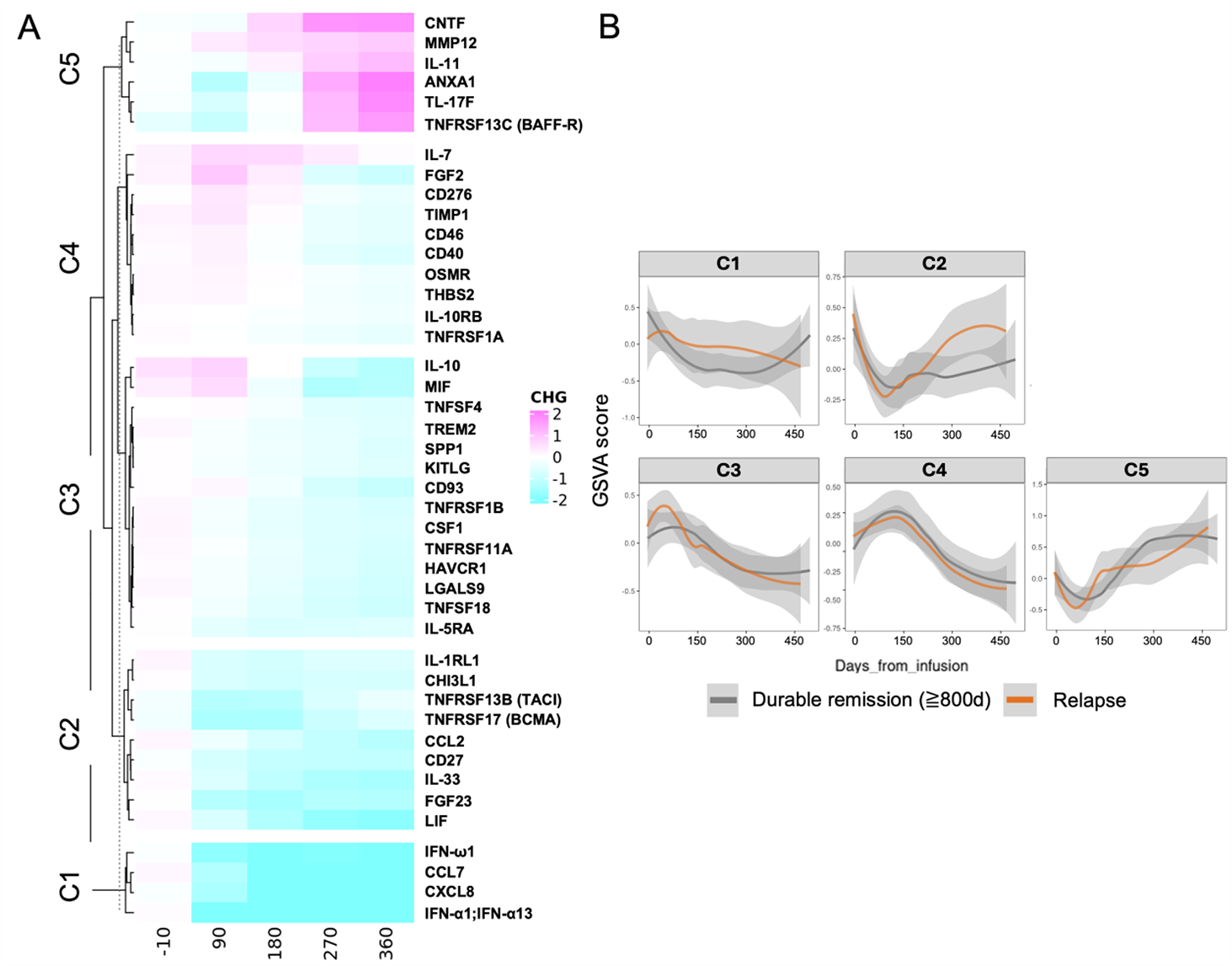
Results: For the DR vs relapse comparison, 14/25 participants were included: 8 in durable remission (SLE n=4, SSc n=3, IIM n=1) and 6 who relapsed (SLE n=2, SSc n=2, IIM n=2); 11 relapse-free participants with follow-up <800 days were excluded (SLE n=5, SSc n=5, IIM n=1). Pharmacodynamic analysis of the subjects in durable remission revealed five distinct modules, each exhibiting a distinct temporal trajectory following CD19 CAR-T infusion (Figure 1A). Module C1 featured type-I interferons and chemokines (e.g., IFNω1, IFNα1/13, CCL7, CXCL8), representing an interferon-chemotaxis signature. Module C2 encompassed markers linked to inflammation and alarmins (IL1R1, CHI3L1, CCL2, IL33) and B-cell lineage support (e.g., BAFF/APRIL receptors such as TNFRSF13B/TACI and TNFRSF17/BCMA, and CD27), indicative of monocyte activation and B- and plasma cell support. Module C3 was rich in proteins associated with regulatory and myeloid functions (e.g., IL10, TREM2, SPP1), which are related to macrophage regulation and tissue repair. Module C4 captured lymphoid and stromal signals (e.g., IL7, CD40, OSMR), reflecting T-cell homeostasis and stromal remodelling. Module C5 involved molecules important for Th17 responses, tissue repair, and the survival of naïve or transient B cells (e.g., IL17F, MMP12, TNFRSF13C/BAFF-R). Trajectory analyses showed that Modules C1 and C2 differed significantly between patients in durable remission and those who relapsed (Figure 1B; C1: F=4.2, FDR=0.0278; C2: F=3.8, FDR=0.0278), while Modules C3 through C5 did not display notable differences (FDR>0.4). Notably, C2 levels dropped in both groups after treatment, but only rebounded in patients who eventually relapsed, whereas they stayed low in those with durable remission.
Conclusions: Tracking serum proteomics over time highlights the importance of the interferon-chemotaxis profile (C1) and the monocyte-alarmin/plasma cell support module (C2) in distinguishing patients with durable remission from those who relapse. These results provide new perspectives on the requisites for a successful immune reset and could inform future patient stratification strategies.
Longitudinal serum proteomic modules identified following CD19 CAR-T therapy. Heatmap display of serum proteins showing significant time-dependent dynamics after CD19 CAR-T infusion. Proteins were grouped into five distinct modules (C1–C5) based on hierarchical clustering of their longitudinal trajectories. The biological characterisation of each module includes: C1 , IFN–chemotaxis (innate activation); C2 , Monocyte–alarmin and plasma-cell support; C3 , Macrophage regulatory/repair; C4 , T-cell homeostasis and stromal remodelling; and C5 , Th17–remodelling and peripheral B-cell survival. Representative proteins for each module are indicated.
Figure 1B. Differential longitudinal trajectories of proteomic modules in Durable Remission (DR) versus Relapse. Longitudinal trajectory plots of module activity scores over time (days relative to infusion) for the DR (grey) and Relapse (orange) groups. Trajectories were modelled using spline regression. Modules C1 (IFN–chemotaxis) and C2 (Monocyte–alarmin/plasma-cell support) showed significant differences between groups (FDR < 0.05). Notably, Module C2 levels initially decreased in both groups but subsequently rebounded in patients who relapsed, whereas they remained suppressed in the DR group. Modules C3, C4, and C5 showed no significant divergence between outcomes. Shaded areas represent 95% confidence intervals.
REFERENCES: NIL.
Acknowledgments: NIL.
Disclosure of Interests: Futoshi Iwata: None declared, Patrick G. Gavin AstraZeneca, Danae-Mona Nöthling: None declared, Kirill Anoshkin: None declared, Laura Bucci: None declared, Panagiotis Garantziotis: None declared, Sarah Clarke AstraZeneca, Nicola Ferrari AstraZeneca, Carlo Tur: None declared, Melanie Hagen: None declared, Andreas Wirsching: None declared, Tobias Rothe: None declared, Sascha Kretschmann: None declared, Simon Völkl: None declared, Michael Aigner: None declared, Fabian Müller: None declared, Andreas Mackensen: None declared, Aline Bozec: None declared, Georg Schett BMS, Cabaletta, Janssen, Kyverna, Miltenyl, Novartis, Ricardo Grieshaber-Bouyer AbbVie, Alfastigma, AstraZeneca, Bristol-Myers Squibb, Candid Therapeutics, Cullinan Therapeutics, Epana Bio, Gilead, Kite, Johnson & Johnson, Kyverna Therapeutics, Lilly, Novartis, Pfizer, Sanofi, UCB.