fetching data ... 
Background: Accelerated biological aging has been implicated in a range of age-related disorders, yet its role in the risk of autoimmune diseases remains poorly understood. Prior studies have focused on a limited number of conditions, most notably rheumatoid arthritis and multiple sclerosis, and have typically relied on a single biological aging metric. Moreover, the predominance of cross-sectional study designs has constrained the ability to evaluate temporal relationships between biological aging and autoimmune disease onset.
Objectives: To examine associations between biological aging, assessed using clinical biomarker–based and proteomic-based measures, and autoimmune disease incidence, and to evaluate differences in life expectancy among individuals with autoimmune diseases by biological aging status.
Methods: We analyzed 470,020 UK Biobank participants free of autoimmune diseases at baseline, defined using International Classification of Diseases 9th and 10th codes and self-reported diagnoses. Two analytic samples were defined: Sample A included participants with complete clinical biomarker data (N=470,020), while Sample B comprised a subset with high-throughput plasma proteomic profiling using the Olink Explore platform (N = 48,863). Biological aging was quantified using complementary measures, including clinical biomarker–based metrics (Klemera–Doubal Method [KDM], PhenoAge, and homeostatic dysregulation [HD]) and a proteomics-based aging score (ProtAge). Associations between biological aging measures and incident autoimmune disease were examined using Cox proportional hazards models with restricted cubic splines to assess nonlinearity, estimating hazard ratios (HRs) and 95% confidence intervals (CIs) after adjustment for demographic, socioeconomic, lifestyle, and clinical covariates. Analyses were conducted for any autoimmune disease (N=42) and for the 20 most common incident autoimmune diseases. Among individuals with incident autoimmune disease, flexible parametric survival models were used to estimate age-specific survival from 45 to 100 years. Remaining life expectancy and years of life lost were calculated by comparing individuals with accelerated versus non-accelerated biological aging. Bonferroni correction accounted for multiple comparisons.
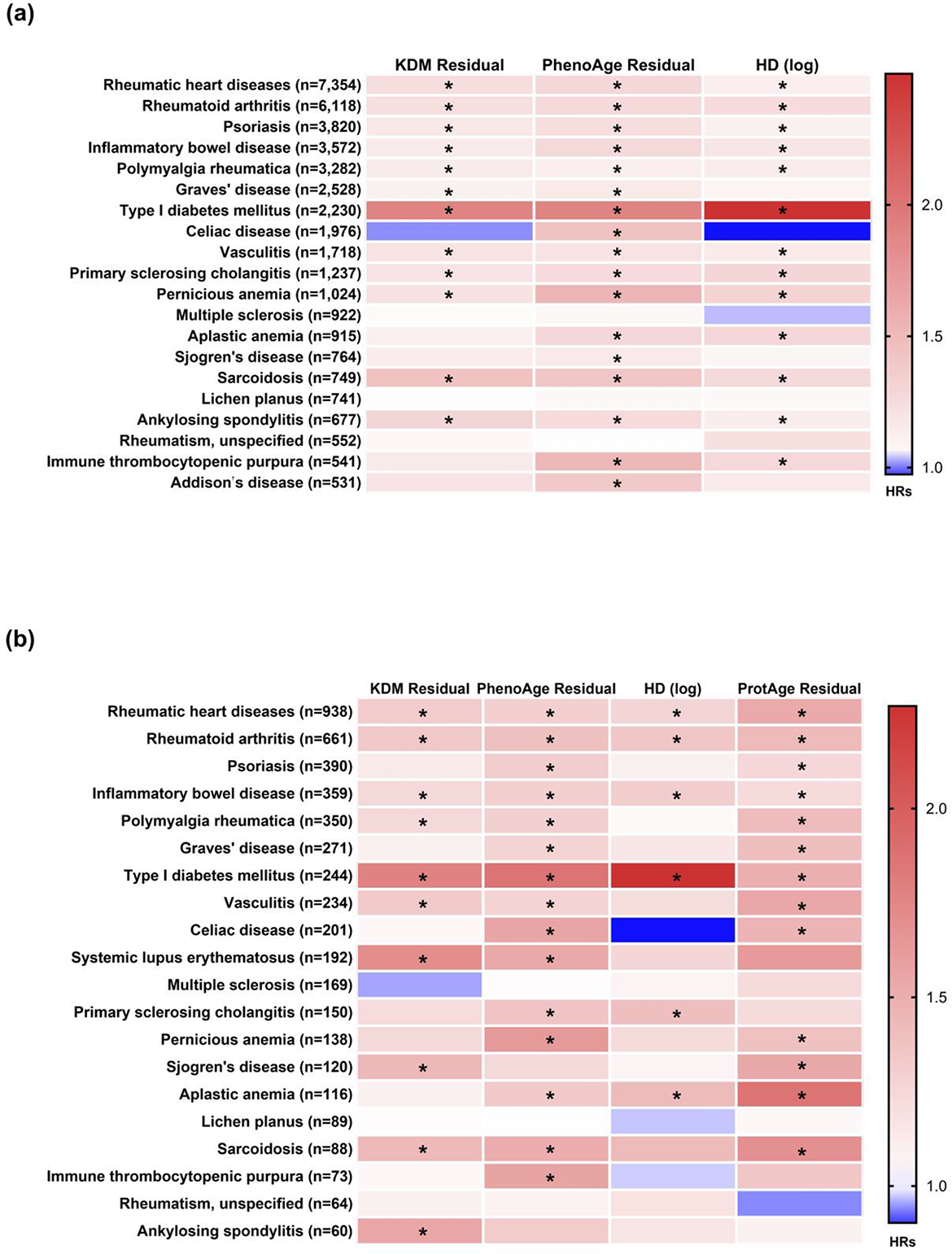
Results: During a median follow-up of 12.7 (Sample A)/12.5 (Sample B) years, 38,169 participants in Sample A (54% female) and 4,437 participants in Sample B (53% female) developed at least one autoimmune disease. A 1-SD increase clinical biomarker-based aging measures was associated with higher autoimmune disease incidence in Sample A (KDM HR 1.19, 95% CI 1.18–1.21; PhenoAge HR 1.28, 95% CI 1.26–1.29, HD HR 1.20, 95% CI 1.18–1.21). Similar associations were observed in Sample B for KDM (HR 1.20, 95% CI 1.16–1.25), PhenoAge (HR 1.29, 95% CI 1.25–1.32), HD (HR 1.21, 95% CI 1.16–1.26) and ProtAge (HR 1.34, 95% CI 1.30–1.38). Restricted cubic spline analyses showed nonlinear associations, with minimal differences at younger biological ages and markedly steeper increases in incidence at higher values for KDM, PhenoAge, and ProtAge. Associations with HD were weaker, largely linear. Substantial heterogeneity was observed across autoimmune diseases across autoimmune diseases, with HRs ranging from 1.10 (95% CI 1.04–1.15; Graves’ disease/KDM) to 2.50 (95% CI 2.38–2.62; type I diabetes mellitus/HD) in Sample A, and from 1.22 (95% CI 1.10–1.35; inflammatory bowel disease/ProtAge) to 2.27 (95% CI 1.95–2.64; type I diabetes mellitus/HD) in Sample B. Among individuals with autoimmune diseases, accelerated biological aging was associated with greater years of life lost. At age 45, estimated years of life lost ranged from 1.2 years for KDM to 4.4 years for PhenoAge in Sample A, and from 2.5 years (KDM) to 6.4 years (PhenoAge) in Sample B, with similar patterns observed at older ages.
Conclusions: In a large prospective cohort, accelerated biological aging, captured via both clinical chemistry and proteomic signatures, was a robust and independent predictor of autoimmune disease incidence across a broad spectrum of conditions. Our study demonstrates that biological age—rather than chronological age—is a significant driver of immune system failure and subsequent mortality. These findings suggest that biological aging metrics could serve as valuable integrative markers for identifying high-risk individuals during the “pre-clinical” window. Furthermore, the link between accelerated aging and autoimmune burden warrants the exploration of geroprotective interventions to slow the “biological clock” as a means of disease prevention. Ultimately, incorporating biological age into clinical assessments could significantly enhance personalized risk stratification and improve long-term prognosis for individuals at risk of, or living with, autoimmune diseases.
Heatmap of associations between biological aging and incidence of top 20 h individual autoimmune diseases in (a) Sample A and (b) Sample B ( HR: Hazard Ratio, * Significant at Bonferroni cut-off )
REFERENCES: NIL.
Acknowledgments: NIL.
Disclosure of Interests: None declared.