fetching data ... 
Background: CD19-CAR T cell therapy is an innovative strategy to induce profound B cell depletion in patients with refractory autoimmune diseases, allowing to reach a sustained drug free remission. Its effects on immune cell phenotypes and transcriptome remain largely unknown.
Objectives: To characterize changes in immune cell subsets and transcriptomic profile in three patients with juvenile dermatomyositis (JDM) and two patients with childhood-onset systemic lupus erythematosus (cSLE) treated with anti-CD19 CAR T cell therapy.
Methods: Three patients with refractory JDM and two patients with refractory cSLE received a single infusion of autologous, second-generation anti-CD19 CAR T cells. Immune cell phenotyping in peripheral blood and bone marrow (BM) samples was performed according to standard operating procedures (SOPs) before (T0) and up to one year after CAR T cell infusion (T1 through T12). IL-10 production by B cells was evaluated in vitro after 72h stimulation with CpG and recombinant CD40L. RNA was extracted from whole blood and depleted from globin and rRNA. Stranded libraries were sequenced on a paired-end run on a NextSeq550 (Illumina). For RNA seq analysis three patients with JDM and three patients with cSLE on standard therapy were included as disease controls. Three adolescents without autoimmune diseases were used as controls.
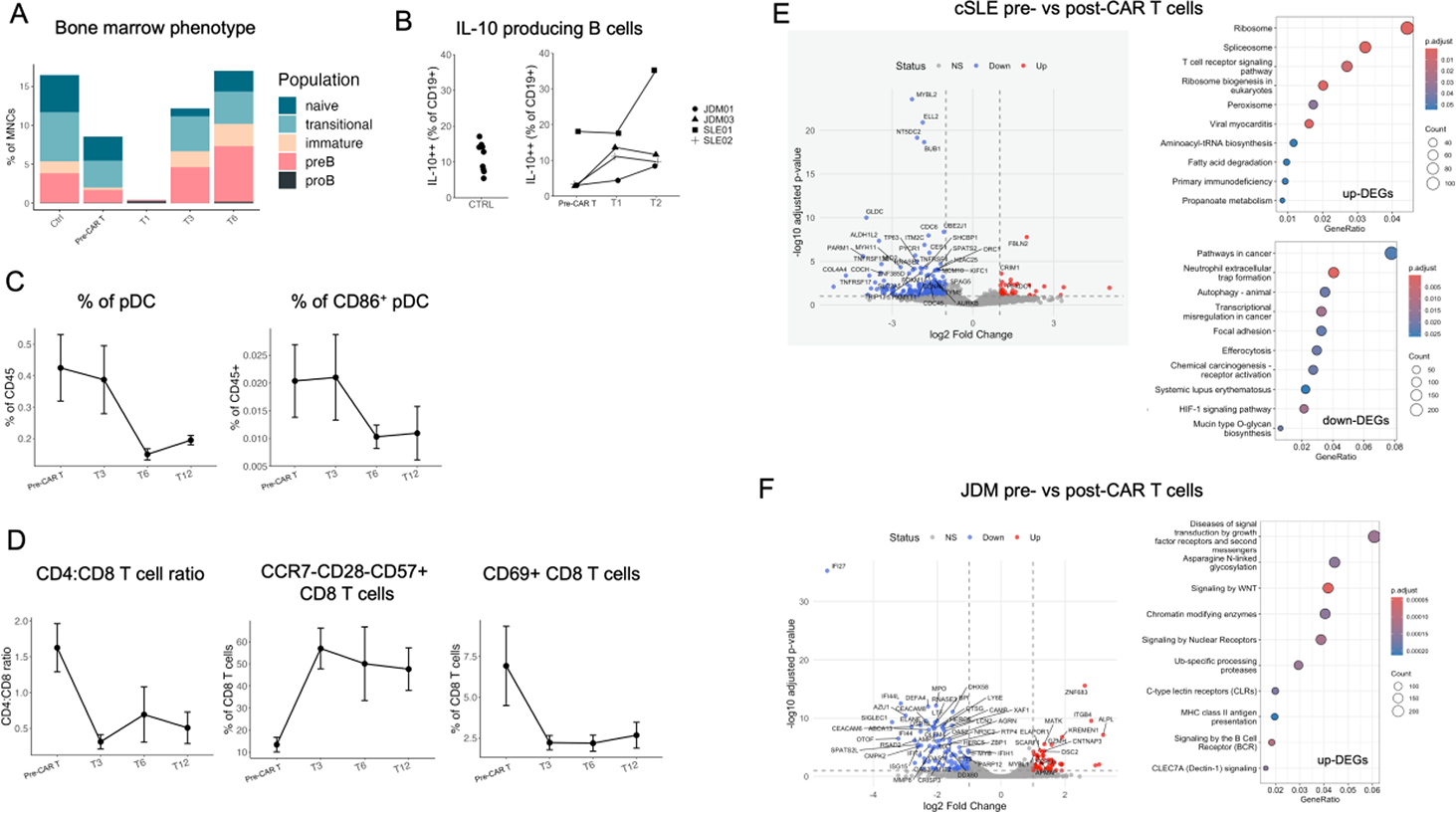
Results: All patients achieved and maintained clinical remission off medication following CAR T cell treatment as previously described (Becilli et al., Nature Medicine 2026). We analyzed B cell reconstitution in the BM for the first six months and in peripheral blood for up to one year after treatment. In BM, B cell depletion was achieved after CAR T cell infusion and reconstitution started from B cell progenitors (pro-B cells and pre-B cells), followed by immature, transitional and naïve B cells (Figure 1A). In peripheral blood, the first B cells to emerge had a transitional phenotype, followed by naïve B cells. Unswitched memory B cells started to reconstitute 6 months after treatment, whereas switched memory B cells were absent up to 12 months after treatment. We compared the B cell phenotype of JDM patients treated with CAR T cells with 10 JDM patients 6 months after rituximab treatment: all patients with CAR T cell treatment reconstituted at 6 months whereas patients treated with rituximab exhibited profound B cell aplasia. The fraction of B cells producing IL-10 assessed in two JDM patients and two cSLE patients was reduced in patients compared to controls and it increased in both cSLE and JDM patients following CAR T cell treatment (Figure 1B). We evaluated the frequency of total pDC and activated CD86+ pDC and we observed a reduction in these populations following CAR T cell treatment (Figure 1C). The ratio of CD4:CD8 T cells decreased after treatment and remained low throughout follow-up. Analysis of T cell phenotypes revealed changes in the CD8 compartment with expansion of terminally differentiated CCR7-CD28-CD57+ CD8 T cells and a reduction in activated CD69+ CD8 T cells (Figure 1D). A total of 318 differentially expressed genes (DEGs) were identified (FDR < 0.1) in cSLE patients before and after CAR T cell treatment, of which 67 were up-regulated and 251 down-regulated in the post-treatment phase (Figure 1E). Both longitudinal pre- vs post-CAR T comparisons and cross-sectional comparisons with responders to standard therapy revealed a consistent downregulation of interferon and complement signatures, together with an upregulation of metabolic and ribosomal pathways (Figure 1E). Additional comparisons with healthy controls further highlighted the distinct molecular impact of the two therapeutic strategies: standard-therapy patients retained interferon activation and showed mitochondrial and chromatin organization defects, whereas CAR T-treated patients exhibited broader suppression of inflammatory, growth, and regenerative pathways. For JDM patients, the direct comparison between samples before and after CAR T therapy allowed the identification of 279 DEGs (FDR < 0.1), of which 120 were up-regulated and 159 down-regulated (Figure 1F). Differential expression analysis highlighted downregulation of interferon-stimulated genes (IFI44L, ISG15, IFI27, SIGLEC1, OAS2) post-CAR T. Conversely, up-regulated genes were enriched for pathways of growth factors, nuclear organization and immune-regulation. In the comparison between CAR T-treated JDM patients and standard-therapy responders (all treated with rituximab), several upregulated genes, including CD22 and CD19, were associated with enrichment in B cell receptor signaling and activation pathways. These results are consistent with the reconstitution of naïve and transitional B cells after CAR T infusion and continuous peripheral B cell depletion in JDM patients treated with rituximab. BloodGen3Module analyses reinforced these observations, showing suppression of interferon and plasmablast modules across both cSLE and JDM cohorts post-CAR T.
Conclusions: In conclusion, CD19-CAR T cell therapy emerges as a powerful disease-modifying approach, capable of achieving deep, durable, and drug-free remissions in children with refractory autoimmune diseases. CAR T cell therapy allowed the reconstitution of a naïve B cell repertoire and restored the regulatory functions of B cells. CAR T cell treatment modulated other relevant immune cells, such as pDC. Terminally differentiated CD8 T cells expanded and activated CD8 T cells decreased after treatment. Transcriptomic analysis revealed a modulation of the interferon module and of metabolic pathways that could be associated with remission. Metabolic assays are undergoing to confirm the metabolic rewiring induced by CAR T cells in patients with autoimmune diseases.
REFERENCES: NIL.
Acknowledgments: NIL.
Disclosure of Interests: Emiliano Marasco BMS, Andrea Ariolli: None declared, Nina De Franco: None declared, Rebecca Nicolai: None declared, Claudia Bracaglia: None declared, Sabina Barresi: None declared, Marco Becilli: None declared, Pietro Merli Personal fees from Sobi, Miltenyi, and Amgen., Maria Isabella Petrone: None declared, Francesca Del Bufalo: None declared, Mattia Algeri Speaker honoraria from Miltenyi Biotec and Raumedic., Consulting fees from Miltenyi Biotec; expert testimony payments from RUHR-IP; travel support from Miltenyi Biotec; material support from Miltenyi Biotec., Research grants from Miltenyi Biotec and Kyverna., Maria Giuseppina Cefalo: None declared, Franco Locatelli Speaker for Miltenyi Biomedicine, Amgen, Novartis, Bristol Myers Squibb, Gilead, MEDAC, and SOBI., Scientific advisory board member for Amgen, Novartis, Sanofi, and Vertex., Fabrizio De Benedetti Member of the Data Safety Monitoring Board for Regeneron; consultant for Sobi, Novartis, and Apollo., Unrestricted research grants from Sobi, Sanofi, Regeneron, Roche, Elixiron, and Novartis.