fetching data ... 
Background: In most Psoriatic Arthritis (PsA) patients [1], psoriatic skin manifestation precedes articular involvement, with ~30% of psoriasis (PsO) patients developing PsA. Arthralgia – joint pain without overt arthritis – identifies patients at high risk of this transition. Fibroblasts are key stromal cells in both skin and synovium that regulate tissue structure, inflammation, and extracellular matrix dynamics and may play a crucial role in transition from PsO to PsA; however, mechanisms and biomarkers of this transition are unknown. Provision of mechanistic insights and the identification of biomarkers would lead to earlier diagnosis and potentially prevention of PsA.
Objectives: To profile skin and synovial fibroblast populations from Psoriasis with Arthralgia (PsO-Arthralgia) and PsA using single-cell RNA sequencing (scRNA-seq) and compare their transcriptional programs to uncover shared pathogenic signatures.
Methods: Slow-frozen skin biopsies (4 mm punch) from lesional (affected) and non-lesional (unaffected) sites and slow-frozen ultra-sound guided synovial biopsies were thawed, washed, minced, and enzymatically dissociated using dispase/DNase. Skin biopsies were further digested with collagenase and trypsin. Resulting skin and synovial cell suspensions were stained with live/dead dye, anti-CD235a, and hashtag antibodies before FACS sorting and counting prior to scRNAseq (10x Genomics 3’ v3.1). Gene expression matrices were processed in Seurat with doublet removal (scDblFinder/DoubletFinder/genotype-based), n-MAD QC filtering, SoupX ambient RNA removal, STACAS integration, and downstream clustering. Differential expression was performed using Seurat’s FindMarkers (MAST), with sample IDs as covariates. Pathway analysis used clusterProfiler, and gene signature scores were calculated with UCell.
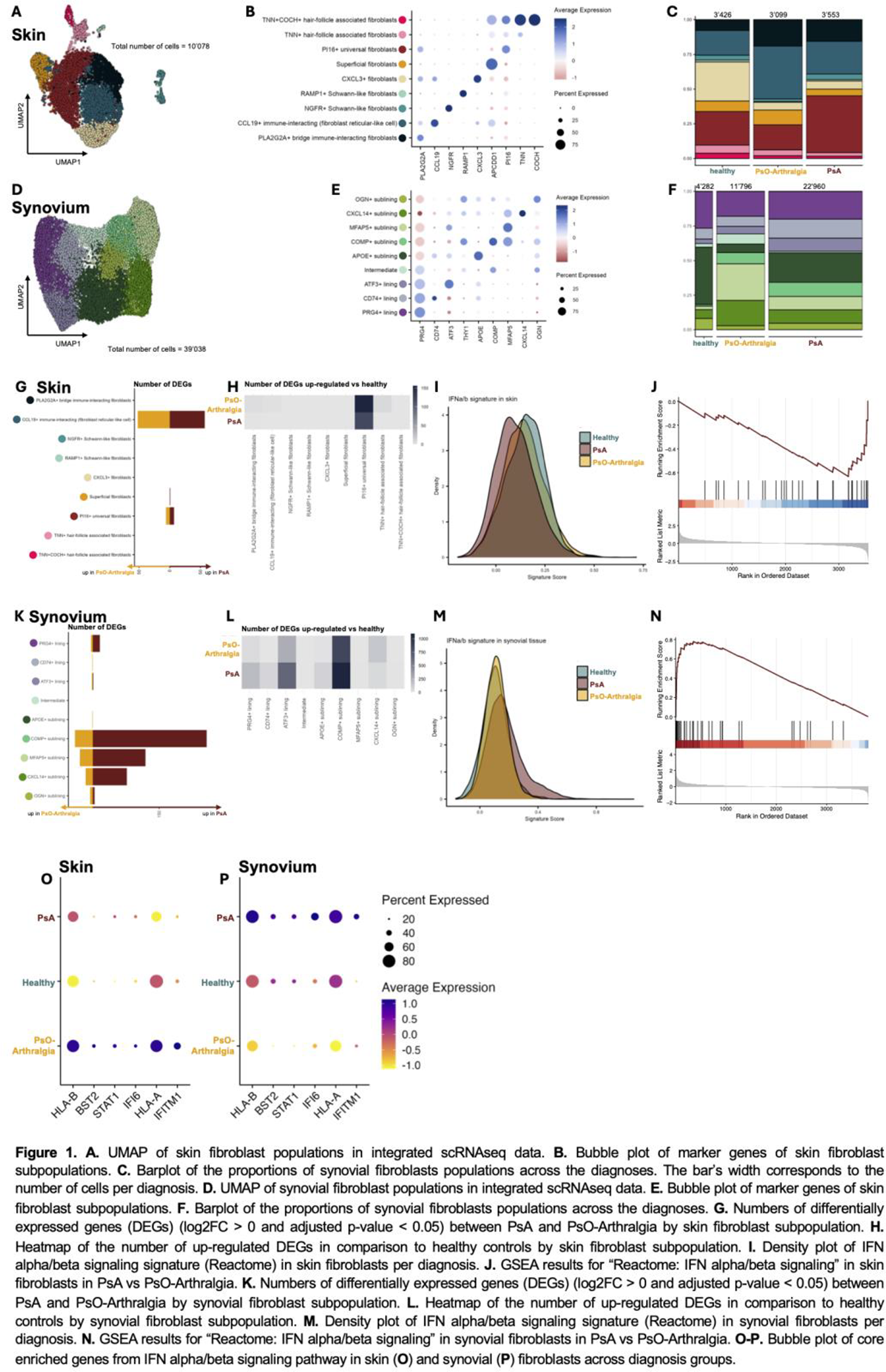
Results: We performed scRNA-seq on skin (n = 34) and synovial biopsies (n = 22) (5 skin/synovium paired samples), including healthy controls for both tissue datasets (skin n = 7, synovial tissue n = 8). Unsupervised clustering and UMAP projection revealed distinct transcriptional compartments corresponding to major cell types. These clusters were annotated based on canonical marker genes, enabling the identification of keratinocytes (KRT5, KRT14; skin-specific), melanocytes (TYRP1, MLANA; skin-specific), fibroblasts (COL1A1, DCN), endothelial and lymphatic endothelial cells (VWF, PROX1), infiltrating immune cells including T cells (CD3D, CD3E), B cells (MS4A1, CD79A), myeloid cells (LYZ, C1QA), and proliferating cell populations (MKI67, STMN1). To further analyze skin fibroblasts across healthy, non-lesional, and lesional skin, we performed subclustering and unsupervised clustering of fibroblast subpopulations. We identified several fibroblast subpopulations: immune-interacting (fibroblast reticular-like cell, CCL19 + and PLA2G2A+), CXCL13 + fibroblasts, Schwann-like fibroblasts (NGFR+ and RAMP1+), superficial fibroblasts (APCDD1+), universal (PI16+), and hair-follicle associated fibroblasts (TNN+ and TNN+COCH+) ( Figure.1A-B ). CCL19 + and PLA2G2A+ immune-interacting fibroblasts showed an increased abundance in both PsA and PsO-Arthralgia patients compared to healthy skin ( Figure.1C ). Analysis of synovial fibroblasts identified three lining (PRG4+, CD74+ and ATF3+), one intermediate (PRG4-low) and five sublining subpopulations (APOE+, COMP+, MFAP5+, CXCL14+, and OGN+) ( Figure.1D-E ). The proportions of these fibroblast subpopulations were comparable between patient groups and healthy controls ( Figure.1F ).
To investigate transcriptional differences across fibroblast subpopulations, we performed differential expression analysis. The CCL19+ immune interacting fibroblasts showed the largest transcriptional differences between PsA and PsO-Arthralgia skin ( Figure.1G ), while PI16+ fibroblasts showed distinct gene expression patterns between patient groups and healthy controls ( Figure.1H ). Notably, all skin fibroblasts, but most prominent the CCL19+ subpopulation, showed, showed down-regulation of IFN alpha/beta signalling pathway in PsA in comparison to both PsO-Arthralgia and healthy (NES = -2.04, p-value < 0.001) ( Figure.1I-J ). Among synovial fibroblast populations, the COMP + sublining fibroblasts exhibited the largest number of transcriptional changes, both in the comparison of PsA versus PsO-Arthralgia ( Figure.1K ) and in the comparison of diseased groups versus healthy controls ( Figure.1L ). Similar to skin fibroblasts, IFN alpha/beta signalling was significantly altered in synovial fibroblasts between PsA and PsO-Arthralgia ( Figure.1M-N ). However, this pathway was up-regulated in PsA compared to PsO-Arthralgia contrasting the results in the skin (NES = 2.25, p < 0.001). Analysis of the core enriched genes from IFN alpha/beta signalling pathway in both skin and synovium identified that the most differentially regulated genes (HLA-A, HLA-B, BST2, STAT1, IFI6, and IFITM1) showed a divergent expression pattern in skin compared to synovial tissue ( Figure.1O-P ).
Conclusions: By mapping skin and synovial cellular landscapes using scRNAseq in PsO-Arthralgia, PsA, and healthy individuals, we identified fibroblast subpopulations with disease-specific transcriptional signatures, including opposing IFN alpha/beta pathway regulation in skin and synovium, that may represent early mechanistic drivers of progression from PsO-Arthralgia to PsA.
REFERENCES: [1] Zabotti et al. EULAR points to consider for the definition of clinical and imaging features suspicious for progression from psoriasis to psoriatic arthritis. Ann Rheum Dis. 2023. doi: 10.1136/ard-2023-224148.
Acknowledgments: NIL.
Disclosure of Interests: Aleksandra Khmelevskaia: None declared, Lavinia Agra Coletto: None declared, Domenico Somma: None declared, Stefano Alivernini: None declared, Mariola Kurowska-Stolarska: None declared, Caroline Ospelt: None declared, Raphael Micheroli UCB, Eli Lilly, Johnson & Johnson, and AbbVie.