fetching data ... 
Background: Symptomatic rheumatoid arthritis-associated interstitial lung disease (RA-ILD) affects ~10% of RA patients and is a leading cause of RA-related mortality. There is a critical unmet need for early biomarkers and effective therapies for RA-ILD. RA-ILD lungs are enriched with B and T lymphocytes that often organize into tertiary lymphoid structures (TLS), which are thought to be pathogenic given their proximity to sites of autoantibody production, fibrosis, and citrullination. While the underlying mechanisms are poorly understood, our single-cell RNA sequencing revealed an increased frequency of CD4 + CXCL13 + T cells that were predominantly CXCR5- in RA-ILD lungs, a phenotype consistent with T peripheral helper cells (Tph). Despite their known role in the synovium, the phenotype, spatial organization, and function of Tph in the lung remain unknown. In this study, we use immunofluorescence (IF) to determine whether lung Tph localize within and outside of TLS/organized lymphoid aggregates in human RA-ILD lung explants.
Objectives: To compare the frequency of Tph within different immune infiltrates in RA-ILD compared to non-RA connective tissue disease (CTD)-ILD and idiopathic pulmonary fibrosis (IPF) and to evaluate the correlation of rituximab treatment of RA-ILD patients with frequency of Tph, CD20+ B cell and different types of immune infiltrates in lung explants.
Methods: Formalin fixed paraffin embedded explanted lung tissues were obtained from patients with RA-ILD (n=11), non-RA CTD-ILD (n=8) or IPF (n=8). IF staining for CD3, CD20 and CXCL13 was completed. To ensure an unbiased analysis, we developed a QuPath pipeline based on established pathology standards to measure immune infiltration. This automated approach was supplemented by a blinded manual count of CD3 + CXCL13 Tph.
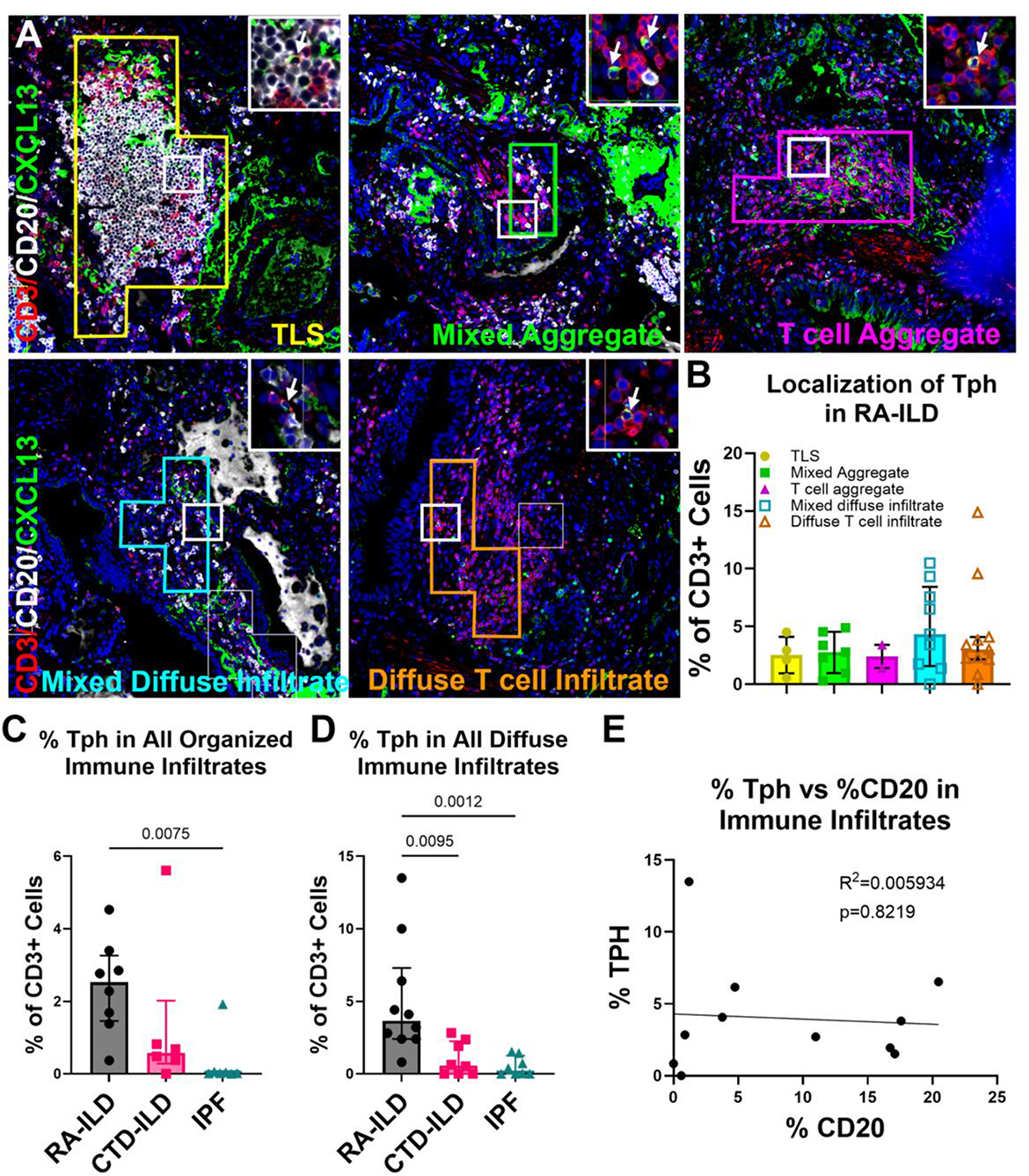
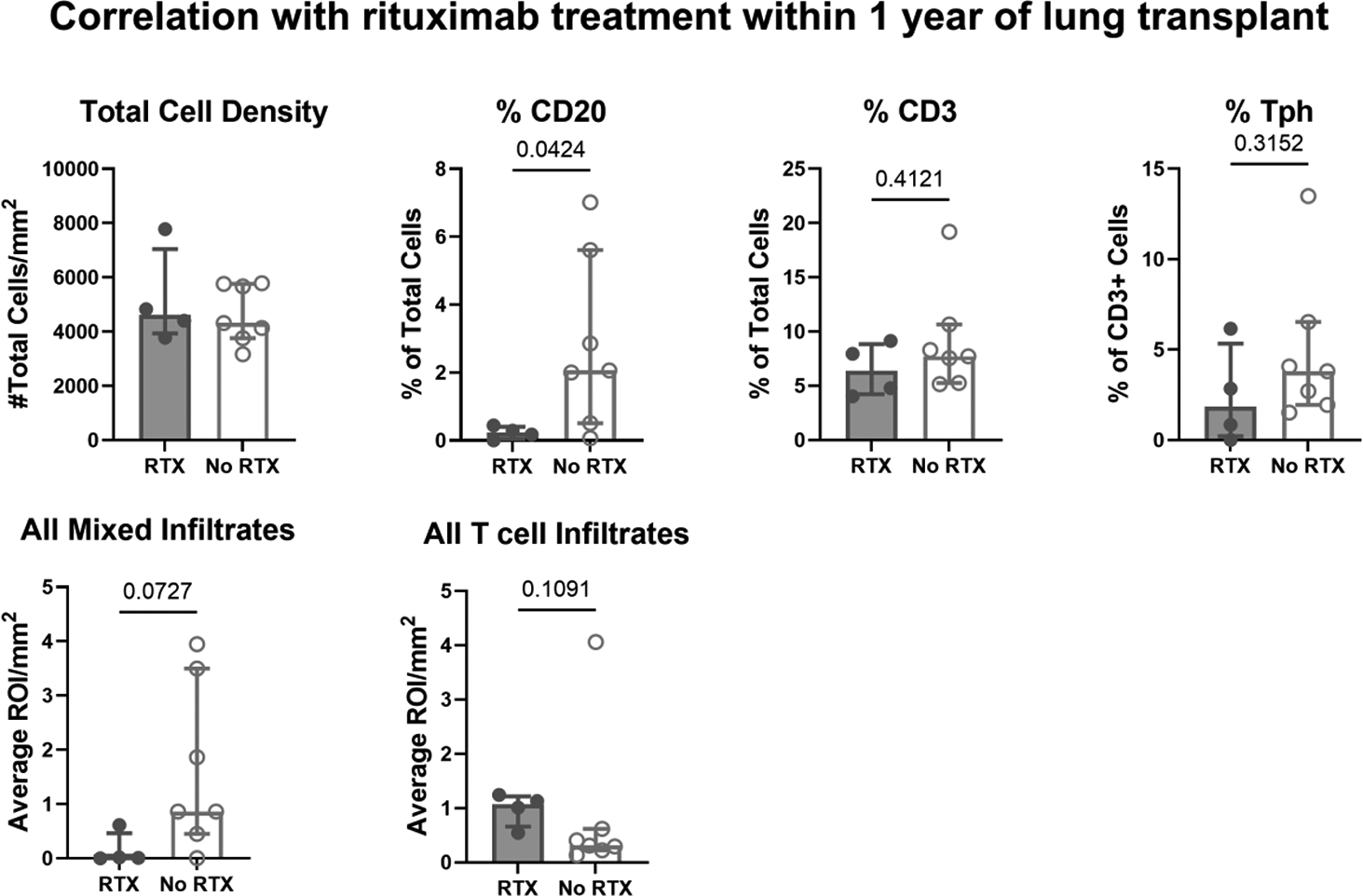
Results: Using IF, we identified Tph within mature TLS as well as in 4 additional types of mixed B and T cell and T cell-predominant immune infiltrates in RA-ILD lung explants: Mixed Aggregate, T cell aggregate, Mixed diffuse infiltrate, T cell diffuse infiltrate (Figure 1A). Tph were present equally in all 5 infiltrate types (Figure 1B). We then compared the frequency of Tph in all organized (combination of TLS, mixed and T cell aggregates) and all diffuse (combination of mixed and T cell diffuse infiltrates) immune infiltrates in RA-ILD, non-RA CTD-ILD and IPF. RA-ILD lungs compared to IPF lungs were significantly enriched with Tph in both organized (median 2.53% vs 0.020%, p=0.0075) and diffuse immune infiltrates (median 3.65% vs 0.21%, p=0.0012) (Figure 1C). When compared to non-RA CTD-ILD, there was a higher frequency of Tph in diffuse immune infiltrates in RA-ILD lungs (median 3.65% vs 0.58%, p=0.0095) (Figure 1C). The presence of Tph in an immune infiltrate in RA-ILD lungs did not correlate with the percentage of CD20+ B cells within the infiltrate (Figure 1D). Additionally, we found that in patients who received RTX treatment within 1 year of transplant correlated with a decrease in CD20 + B cell frequency (0.23% vs 2.06%, p=0.04), a non-significant trend towards less CD20 + B cell-containing immune infiltrates per mm 2 (median 0.01 vs 0.87, p= 0.07) (Figure 2). Notably, no significant change in Tph frequency was observed (Figure 2).
Conclusions: These results demonstrate that increased frequency of Tph is unique to RA-ILD lung explants compared to non-RA CTD-ILD and IPF and that Tph can be found both in organized and diffuse immune infiltrates in RA-ILD lung explants. Interestingly, despite being predominantly known for B-cell helper functions, Tph frequency did not correlate with the presence of B cells and Tph were found in CD20-depleted RA-ILD lung explants. These findings suggest that Tph may have other roles besides B-cell helper functions in RA-ILD pathogenesis and that there may be different subsets of Tph in the RA-ILD lung, such as those the RA synovium. Future directions include spatial transcriptomics to determine whether distinct Tph subsets localize to different immune infiltrates and lung microenvironments and single cell sequencing to identify specific Tph pathways in RA-ILD lung explants. Further evaluation of the mechanisms behind Tph-mediated RA-ILD pathogenesis could reveal novel biomarkers and therapeutic targets for RA-ILD.
Frequency of Tph in different immune infiltrates in RA-ILD, other CTD-ILD and IPF lung explants. A ) Representative IF images of different immune infiltrates. The white inset and zoomed square represent a 40X magnified area (white arrows indicate Tph). B ) Average % Tph (# Tph/# CD3) in different immune infiltrates in RA-ILD lung explants. Average % Tph in C ) all organized (combination of TLS, mixed and T cell aggregates) and D ) all diffuse (combination of mixed and T cell diffuse infiltrates) immune infiltrates in RA-ILD, other CTD-ILD, and IPF lung explants. E ) Scatter plot demonstrating the correlation between % Tph and % CD20 (# CD20/ Total # cells) in immune infiltrates. B-E) Each dot represents the average % of the specified cell type from up to 10 images for each immune infiltrate type for 1 patient. B-D) Data are represented as the median ±IQR. p-values<0.05 by Kruskal-Wallis noted above each comparison. E) Simple linear regression.
Correlation of rituximab treatment within 1 year of transplant with the cell frequency and number of immune infiltrates in RA-ILD explanted lungs. All mixed immune infiltrates were a combination of TLS, mixed aggregates and mixed diffuse infiltrates. All T cell immune infiltrates represent a combination of T cell aggregates and diffuse T cell infiltrates. Data are represented as the median ±IQR. p-values <0.5 by Mann-Whitney noted above each comparison. ROI= region of interest.
REFERENCES: NIL.
Acknowledgments: NIL.
Disclosure of Interests: Amara Seng: None declared, Kensuke Suga: None declared, Anvita Singaraju: None declared, Beulah Esther Rani Samuel: None declared, Youn Jung Choi: None declared, Justyna Fert-Bober: None declared, Jon Giles Consultant to AbbVie, Pfizer, Genentech, Eli Lilly, Oruka, Novartis, Tanyalak Parimon: None declared, Peter Chen Consultant over three years ago: Eli Lilly, Regeneron, Gilead, Nunzio Bottini I consult for Merck and Tonix Pharmaceutical.