fetching data ... 
Background: Pregnancy-induced remission of rheumatoid arthritis (RA) and subsequent postpartum flare are common, but underlying immunologic mechanisms remain poorly understood. Existing work is limited by the study of small cohorts of pregnant females with RA, using traditional cellular techniques, lacking longitudinal samples from pre- to post-pregnancy with appropriate controls, thereby limiting the depth and detail of possible analyses.
Objectives: To study, for the first time, longitudinal immunologic changes in peripheral blood before, during and after pregnancy in RA. We analyse a unique, prospectively collected cohort including RA-affected females and healthy controls (HC), using 31-marker spectral flow cytometry.
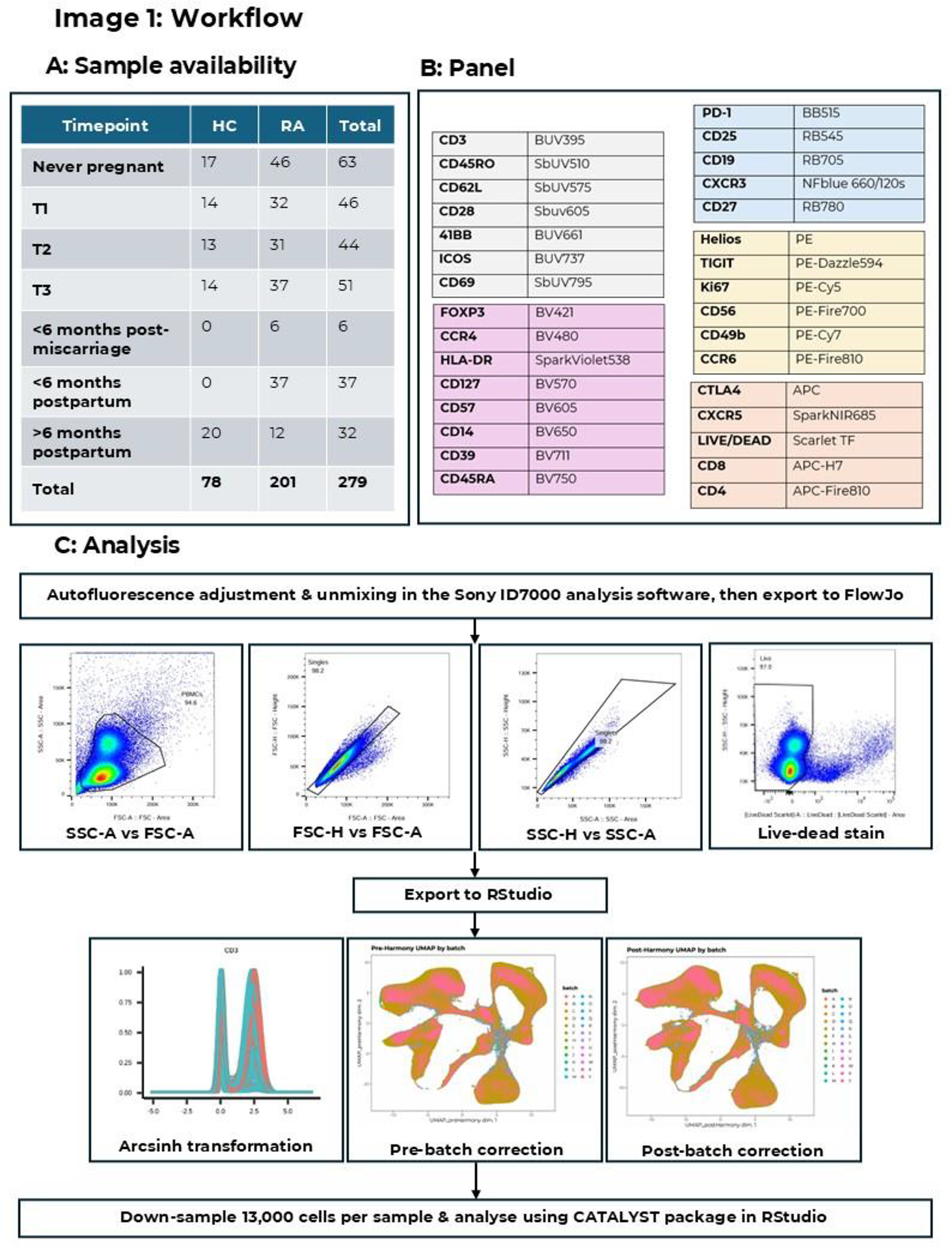
Methods: Females of childbearing age were recruited at University College London Hospital, London, and Erasmus University Medical Centre, Rotterdam. Recruits included pregnancies in participants with RA, with longitudinal samples spanning pre-pregnancy, pregnancy and postpartum, and pregnancies in HC with paired pregnancy and postpartum samples. We also included non-pregnant females of childbearing age without a linked pregnancy. Pregnancy samples were assigned to trimester (1 st , 2 nd , or 3 rd ), and samples from non-pregnant individuals were classified as never pregnant (no prior pregnancy) or, where a prior pregnancy was documented, as postpartum (<6 months or >6 months), Figure 1A.
Peripheral blood mononuclear cells (PBMCs) were analysed using spectral cytometry, Figures 1B-C. Unmixing and autofluorescence adjustment were performed within the Sony ID7000 software. Gating for single, live PBMCs was performed in FlowJo, followed by the remainder of the analysis in RStudio using the Harmony package for batch correction and CATALYST for clustering, differential testing and plotting. An equal number of cells were randomly down-sampled from each participant time point, and cell-type abundance expressed as a percentage of this down-sample (median +/- interquartile range; IQR). Comparisons between RA and HCs were performed using the Mann-Whitney U test (p-value <0.05 for significance). Six samples from RA-affected females collected within 6 months of a miscarriage were retained for clustering but excluded from downstream analyses of cell population change across pregnancy.
Results: In total, 279 samples (n=201 RA, n=78 HC) were obtained from 106 participants (n=67 RA, n=39 HC). Median age at recruitment for RA was 31.9 years (IQR 30-34), and for HC was 31.0 years (IQR 28-34). Among participants with RA, 67.2% (n=45) were seropositive for either rheumatoid factor or anti-cyclic citrullinated peptide, the median disease duration was 4 years (IQR 2.3-8.0), and 9.0% (n=6) were smokers. In comparison, 7.7% (n=3) of controls were smokers. Median age was 30.5 years (IQR 27–33) in never-pregnant samples and 34.0 years (IQR 31–39) in samples collected >6 months postpartum.
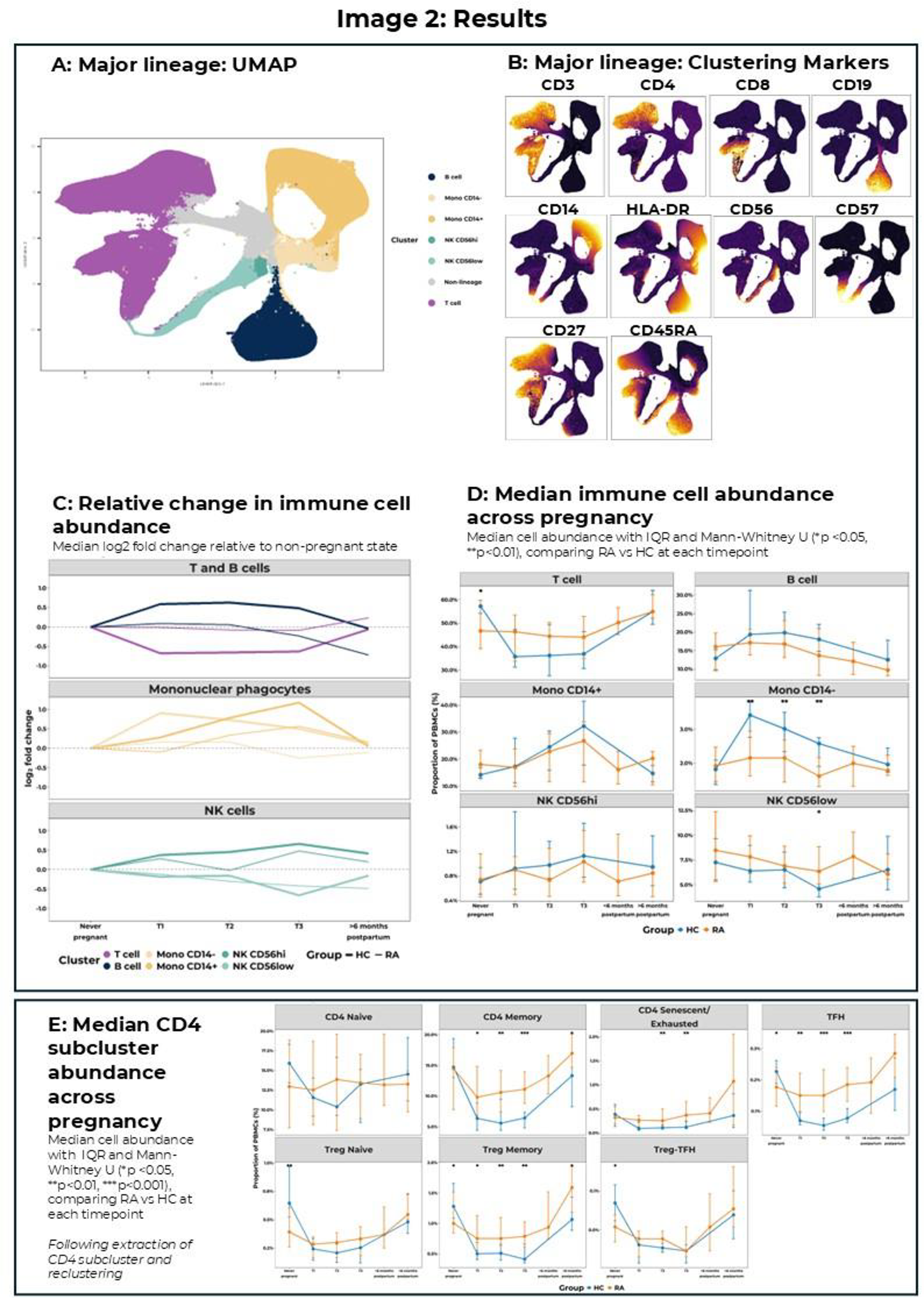
Major cell populations were identified by clustering on CD3, CD4, CD8, CD19, CD14, HLA-DR, CD56, CD57, CD27 and CD45RA, Figures 2A-B. Differential alterations in the abundance of major lineage populations across pregnancies were observed in RA and HCs, Figures 2C-D. Specifically, in healthy participants, peripheral blood T cell abundance was reduced throughout pregnancy and normalised after delivery, Figures 2C-D. HCs also experienced an early increase in B cells and CD14- mononuclear phagocytes, a gradual rise in CD14+ mononuclear phagocytes to a 3rd-trimester peak, and divergent NK cell population trajectories, with CD56hi populations increasing in pregnancy and CD56low populations decreasing. Similar trajectories were observed in participants with RA, but compared to HCs, they experienced less change from non-pregnant baseline, particularly for T cells. Significant differences in major lineage abundance between RA and HC were observed in all three trimesters for CD14- mononuclear phagocytes (lower in RA than HC, p<0.01) and in CD56low NK cells in the 3 rd trimester (higher in RA than HC, p>0.05), Figure 2D.
CD4-positive T cells were sub-clustered for further analysis. Clusters were allocated to one of seven broad groups: CD4 Naïve (CD45RA+, CD27+), CD4 Memory (CD45RA-), CD4 Senescent/Exhausted (CD57+, CD45RA+/-, +/- TIGIT, PD1, CTLA4), T follicular helper (TFH; CXCR5+, PD1+, ICOS+), Regulatory T cell (Treg) Naïve (CD45RA+, CD25hi, CD127low, FOXP3+), Treg Memory (CD45RA-, CD25hi, CD127low, FOXP3+), and Treg-TFH (CD25hi, CD127low, FOXP3+, CXCR5+, PD1+, ICOS+). All CD4 populations were reduced in abundance during HC pregnancy, Figure 2E. In contrast, RA pregnancies showed variable changes in naïve CD4 T cells and an increased abundance of TFH and senescent/exhausted CD4 T cells relative to the non-pregnant baseline. Furthermore, compared with HCs, individuals with RA exhibited a significantly higher abundance of CD4 memory, senescent/exhausted, TFH, and Treg memory cells throughout pregnancy (all p<0.05 in the 2 nd and 3 rd trimesters), Figure 2E.
Conclusions: Pregnancy leads to an increase in peripheral blood abundance of B cells, mononuclear phagocytes, and CD56hi NK cells, and a reduction in T cells and CD56low NK cells. During pregnancy, individuals with RA experience different trajectories relative to controls, tending to have higher T cell abundance, with an increased proportion of antigen-experienced CD4 T cells, including memory cells, senescent/exhausted cells, and TFH cells.
Associations with disease activity, medication use, and clinical phenotype, as well as more detailed cellular analyses, are ongoing. We are also performing proteomic analysis of >1,000 proteins using matched serum samples from all participants. Our goal is to use pregnancy as a model of tolerance and flare – to explore the pathophysiologic mechanisms underpinning these events across pregnancy.
REFERENCES: NIL.
Acknowledgments: NIL.
Disclosure of Interests: Bethan Goulden Talk on lupus pregnancy for GSK, 2024, Bennie van Heeswijk: None declared, Heather Cross: None declared, Luis Fernando Perez: None declared, Esther Röder: None declared, Erik Lubberts: None declared, Elizabeth Jury: None declared, George Robinson: None declared, Radboud J.E.M. Dolhain UCB, Roche, Abbvie, Genzyjme, Novartis, ASTRA Zeneca, Eli LiLy, Unrestricted research grants from:
Dutch Arthritis Association, ZonMw, UCB Pharma, Galapagos, Ian Giles Coauthor on an educational review article in 2020 and speaker fees from UCB, and has participated in advisory boards for UCB. B.G. has received speaker fees from GSK, Unrestricted research grants from Union Chimique Belge (UCB).