fetching data ... 
Background: High circulating anti-cyclic citrullinated peptide (anti-CCP) levels strongly predict progression to inflammatory arthritis (IA) in at-risk individuals, reflecting breach of tolerance to citrullinated antigens [1]. Clonally expanded CD8 + T cells, which recognise and respond to citrullinated autoantigens via MHC class 1, have recently been identified in the blood and synovium of CCP+ RA patients [2]. Whether such clonal expansions arise during the pre-arthritis phase of RA and potentially contribute to the development of arthritis is unclear. We aimed to characterise circulating CD8 + T cell clonal expansion in anti-CCP + at-risk individuals using scRNA sequencing and explore associations with subclinical joint inflammation and progression to clinical arthritis.
Objectives: To define transcriptional states and clonal architecture of circulating CD8 T cells in anti-CCP+ at-risk individuals and determine their relationship to ultrasound (US)- defined subclinical synovitis and progression to clinical arthritis.
Methods: Peripheral blood mononuclear cells were collected from 45 donors in the Leeds CCP cohort (5 healthy controls; 40 CCP+ individuals at risk with arthralgia but without clinical synovitis). Of the 40 CCP+ at risk, 18 did not develop arthritis (non-progressors); of the 22 who later developed arthritis, 11 had no subclinical synovitis (US-negative future progressors) and 11 had subclinical synovitis (US-positive future progressors). All samples underwent paired single-cell RNA sequencing and T-cell receptor (TCR) sequencing. US positivity was power Doppler ≥1 and greyscale ≥1; IA was ≥1 swollen joint confirmed by a rheumatologist. Analyses were performed in R using Seurat and Harmony. Raw gene expression counts were log-normalised, 3,000 variable features were selected, scaled, and reduced by PCA (≈30 PCs). Batch effects (donor/chemistry) were mitigated with Harmony while preserving lineage structure. To emphasise immune lineages over activation, a lineage-aware embedding was recomputed on a fixed marker panel (pan-T, CD4, CD8, B, NK, MAIT, γδ, Treg) and a shared UMAP used for all overlays. The CD8/MAIT/γδ compartment was re-clustered (k-NN on 20 PCs; Louvain, resolution 0.4; k-means k=4 concordant). Program heatmaps used a curated 55-gene panel (cytotoxicity, cytokine/chemokine, activation/exhaustion, naïve/memory, interferon response, residency/MAIT/γδ, transcription factors) with donor-equal summaries by group×clone-class. Clonotypes were defined by TRB CDR3 amino-acid identity; clone sizes per donor were Singleton (1), Small (2–4), Medium (5–19) and Large (≥20). Diversity used Shannon entropy, Pielou evenness and a clonality index (1−H/lnS). Differential expression used Wilcoxon tests with FDR control; TRBV/TRBJ usage was summarised by chord diagrams.
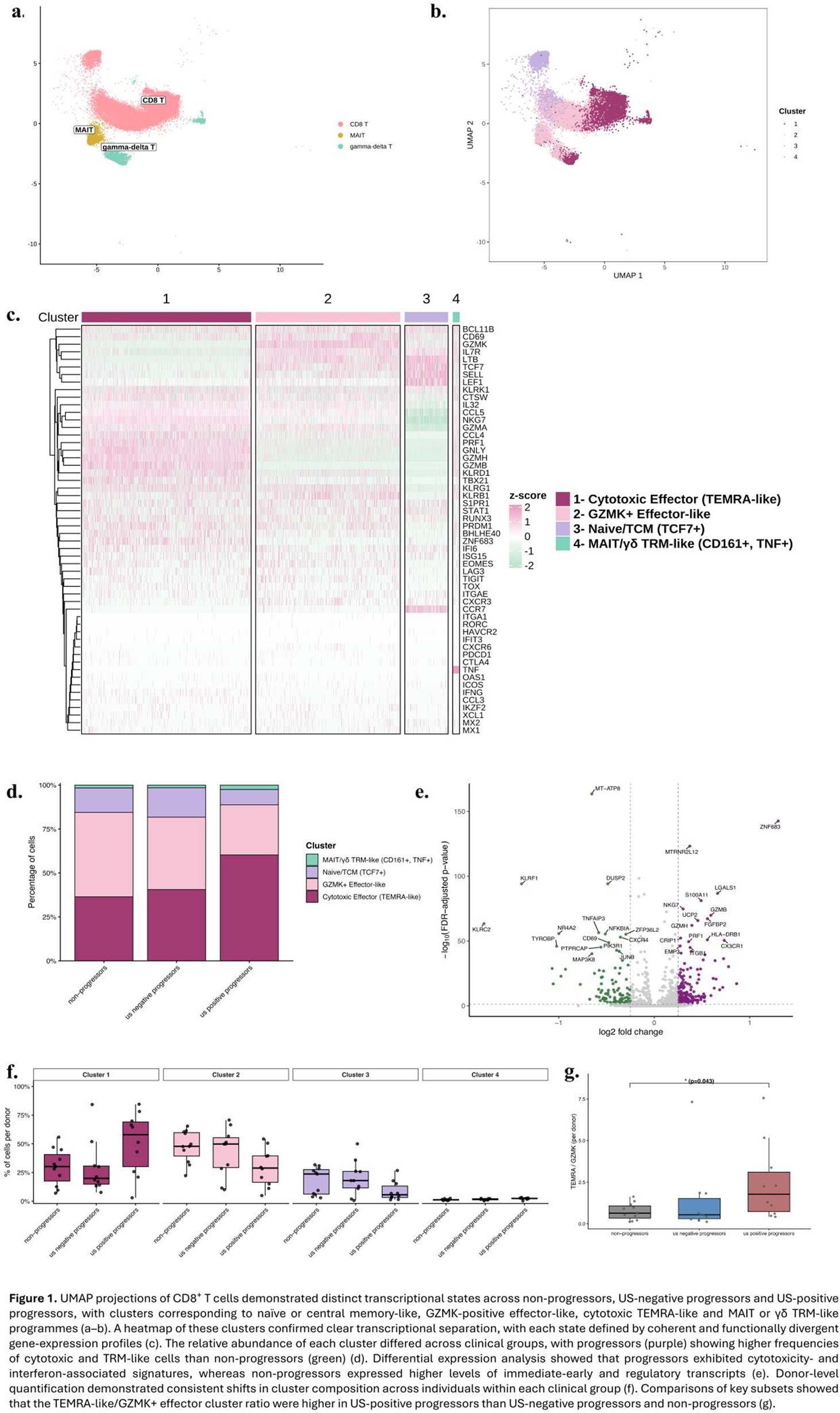
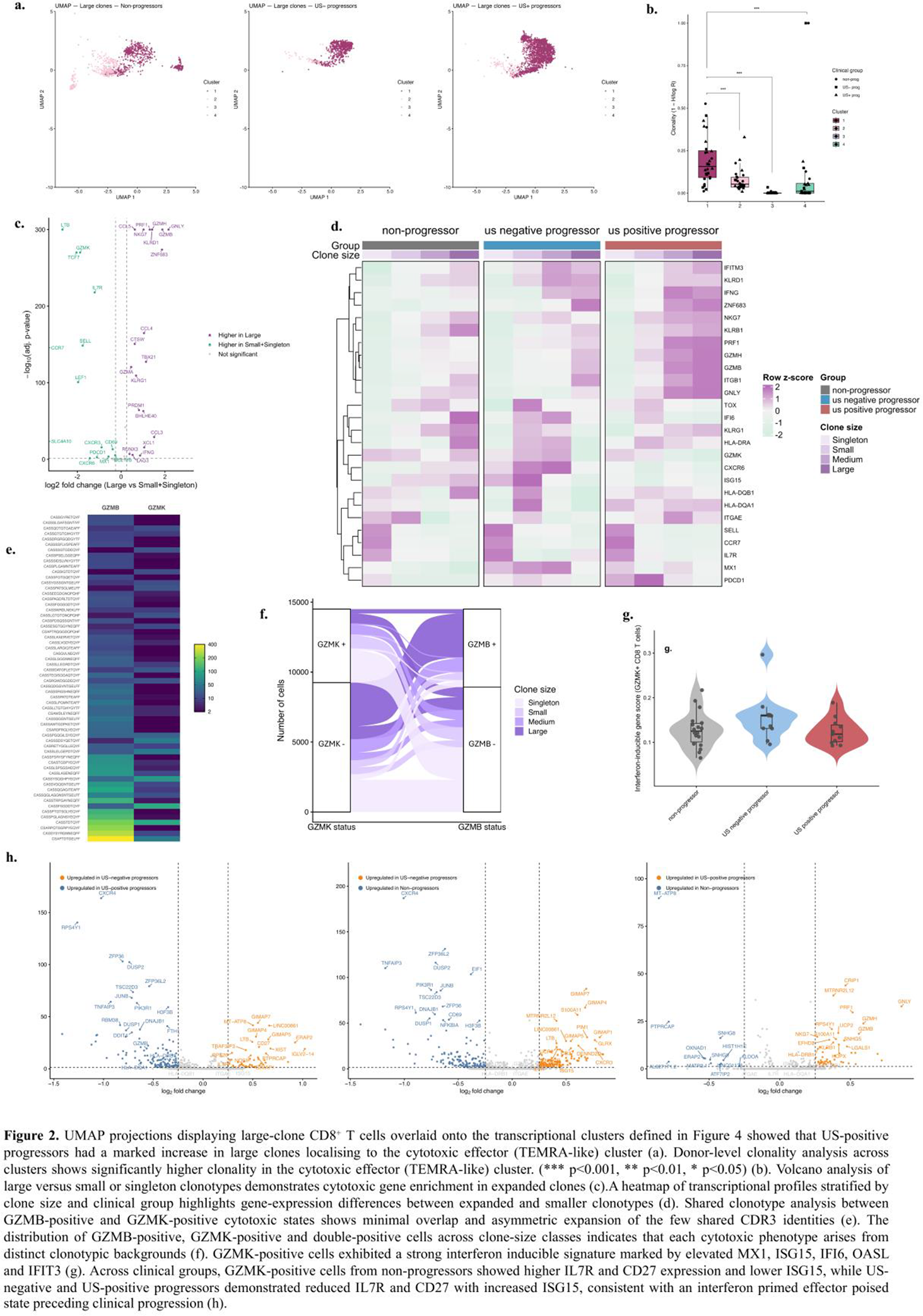
Results: Lineage-aware analysis identified four conserved CD8 programmes: (i) naïve/central memory-like (TCF7, CCR7, IL7R), (ii) GZMK+ effector-like (GZMK, CCL3/4), (iii) cytotoxic TEMRA-like (PRF1, GZMB, GNLY, NKG7), and (iv) MAIT/γδ tissue-resident–like (KLRB1, RORC, ZNF683, ITGAE), forming discrete islands on the shared UMAP and stable graph-based clusters (Figure 1a–c). Clinical stratification showed progressive remodelling: non-progressors were enriched for naïve and GZMK+ cells, whereas US-positive progressors had expanded cytotoxic TEMRA-like and tissue-resident–like populations with contraction of naïve and GZMK+ states (Figure 1d, f). Gene expression shifted from regulatory/immediate-early programmes (DUSP2, JUNB, NR4A2, TNFAIP3) to cytotoxic and residency imprints (PRF1, GZMB, CX3CR1, FGFBP2, ZNF683) after onset of subclinical synovitis (Figure 1e). TCR analysis demonstrated highly non-random clonal expansion concentrated within cytotoxic TEMRA-like regions (Figure 2a). Donor-level clonality increased stepwise from non-progressors through US-negative and US-positive progressors, with reduced entropy indicating growing clonal dominance (Figure 2b). Large clonotypes preferentially expressed cytotoxic/residency genes, whereas singleton/small clones retained naïve/regulatory signatures (Figure 2c, d). Additionally, two CD8 effector programmes were supported by largely distinct clonotypic backgrounds. GZMB+ CD8 T cells were strongly associated with large, expanded clones in US-positive future progressors, marking a late effector phase preceding IA (Figure 2a–d). In contrast, GZMK+ CD8 T cells predominated in US-negative progressors and showed the strongest interferon-primed profile across groups, with higher MX1, ISG15, IFI6, OASL and IFIT3 and reduced IL7R/CD27 compared with non-progressors (Figure 2g, h). Importantly, this IFN-driven GZMK programme in US-negative future progressors was largely non-clonal and enriched in small and medium clone classes rather than in large expanded clonotypes (Figure 2d). Clonotype sharing between GZMK+ and GZMB+ states was minimal, indicating divergent CD8 programmes rather than alternative activation states of the same clones (Figure 2e, f).
Conclusions: In anti-CCP+ individuals at risk of RA, CD8 T-cell immunity evolves through discrete stages. An interferon-primed, largely non-clonal GZMK+ effector state precedes the onset of subclinical joint inflammation when IA is imminent. When subclinical synovitis develops, a clonally expanded, GZMB+ cytotoxic effector phase predominates and immediately precedes clinical arthritis. These data demonstrate the emergence of discrete CD8 T cell effector phenotypes when RA is imminent and suggest a window for immunological interception before persistent arthritis develops.
Transcriptional heterogeneity of CD8 + T cells and differential gene expression across CCP+ at-risk individuals
Clonotype segregation and interferon-driven remodelling of cytotoxic CD8 + T-cell states.
REFERENCES: [1] Duquenne L, et al. Ann Intern Med. 2023 Aug;176(8):1027-1036. [2] Moon JS, et al. Nat Commun. 2023 Jan 19;14(1):319.
Acknowledgments: NIL.
Disclosure of Interests: Kerem Abacar: None declared, Fareeha Tariq: None declared, Paul Martin: None declared, Weiyu Ye: None declared, Xiang Sun: None declared, Sophie MacKay: None declared, Dylan Muldoon: None declared, Laurence Duquenne: None declared, Andrea Di Matteo: None declared, Kate Harnden: None declared, Katie Mbara: None declared, Madhvi Menon: None declared, Hussein Al-Mossawi: None declared, Maya Buch: None declared, Paul Emery AbbVie, BMS, Pfizer, MSD, Roche, Janssen, Novartis and UCB, AbbVie, BMS, Pfizer, MSD, Roche, Darren Newton: None declared, Benjamin Fairfax: None declared, Kulveer Mankia Abbvie, ALLin Bio, Alchemab Thertapeutics, Astra Zeneca, Engitix, UCB, Lilly, Galapagos, Serac Healthcare, Zura Bio, Deepcure, Ventus Therapeutics, Gilead, Lilly, Serac Healthcare, Astra Zeneca, Deepcure, Alfa-Sigma.