fetching data ... 
Background: Rosnilimab is an investigational monoclonal antibody that selectively targets and depletes pathogenic T cells (i.e., PD-1 high Tph/Tfh, Teff). By acting upstream of multiple clinically validated inflammatory pathways in rheumatoid arthritis (RA), rosnilimab represents a potentially distinct therapeutic approach. In RENOIR, a Phase 2B trial of rosnilimab in adults with moderate-to-severe RA (NCT06041269), the primary endpoint of mean change from baseline in DAS28-CRP at Week (Wk) 12 was met by all rosnilimab doses versus placebo. ACR20 and mean change in hs-CRP within 3 months were statistically significant across all doses versus placebo with evidence of durable responses following treatment discontinuation. This trial included longitudinal translational analyses, enabling characterization of molecular profiles in peripheral blood and inflamed synovial tissue before and after rosnilimab treatment.
Objectives: To elucidate the pharmacodynamic and mechanistic effects of rosnilimab in adults with moderate-to-severe RA from a multicenter, randomized, double-blind, placebo-controlled Phase 2B study through peripheral blood flow cytometry and serum protein analyses, as well as synovial tissue histopathology and molecular profiling.
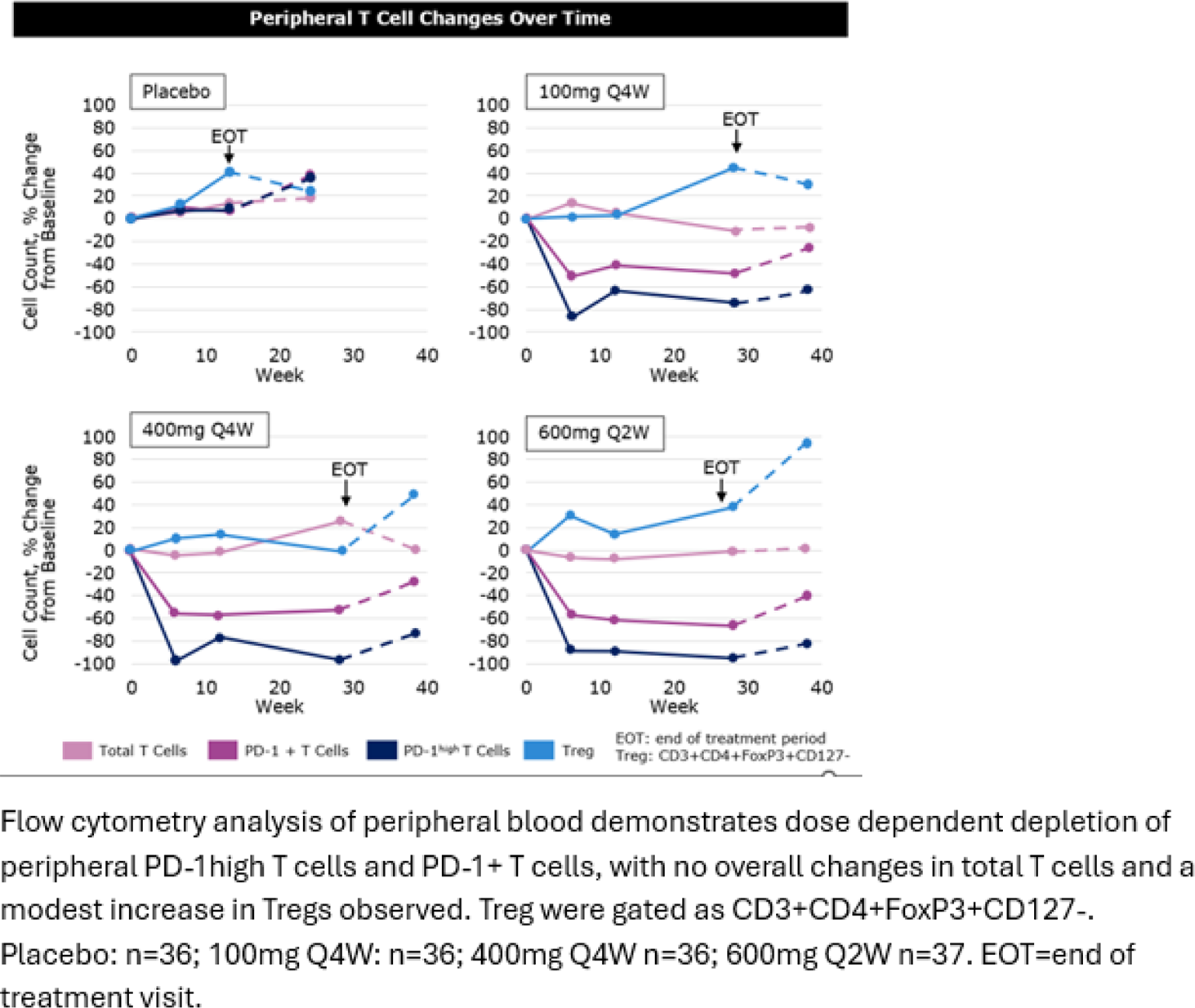
Methods: Blood and serum samples were collected on Day 1 (pre-dose), Wk 6, Wk 12, Wk 28, and Wk 38 (off-drug follow up period). Flow cytometry of peripheral blood quantified total T cells, PD-1+ Teff, regulatory T (Treg) cells (n=145), Tph and Tfh cells (n=132). OLINK proximity extension assays measured serum cytokine and chemokine levels (n=420). Synovial tissue was collected into formalin or RNA later via ultrasound-guided or arthroscopic biopsy on Day 1 and Wk 6. Synovial inflammation was graded from formalin-fixed, paraffin embedded (FFPE), H&E-stained slides using the Krenn synovitis score (n=80 total samples). Bulk RNA sequencing (RNA-seq) (n=24 evaluable paired biopsies) was performed and subsequent transcriptome data were analyzed for differential expression and pathway enrichment using Gene Ontology (GO) sets. Tissue PD-1+ T cells and B cells were quantified by immunofluorescence staining using the Akoya imaging platform (n=39 evaluable paired biopsies). Changes from baseline were calculated from synovial samples containing ≥ 10 cells/mm 2 (T cells) or ≥5 cells/mm 2 (B cells) in the pre-treatment biopsy.
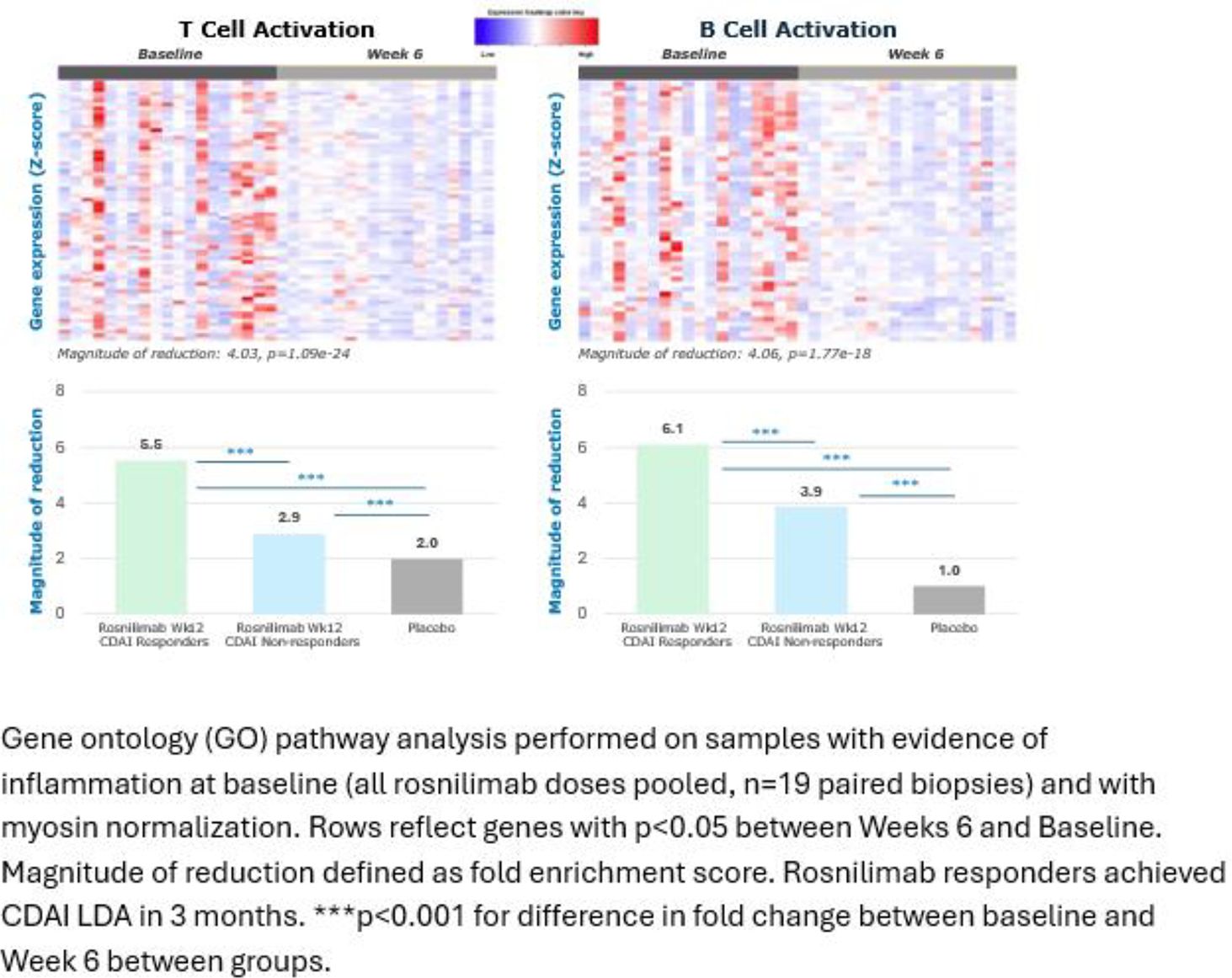
Results: In peripheral blood, rosnilimab reduced PD1+ T cell counts at all doses by approximately 50% and selectively depleted pathogenic T cells (defined by high PD-1 expression), including Tfh, Tph, and activated effector T cell populations by over 90% (p < 0.001) at all timepoints. Notably, there were no significant changes to total T cell numbers, while a modest increase in Tregs at later timepoints was observed (Figure. 1). Pathogenic T cell depletion was accompanied by reductions in key pro-inflammatory serum biomarkers, including CRP (p < 0.01), IL-6, CXCL13, and MCP-3 (p < 0.05). In synovial tissue, Krenn scores at baseline ranged from 0 to 7 in evaluable samples for all dose groups. Paired samples from the 400 and 600 mg dose groups showed a mean reduction of 41% in Krenn scores from Day 1 to Wk 6, while placebo and 100 mg dose groups were unchanged. Rosnilimab treatment resulted in an approximately 90% reduction of synovial PD-1+ T cells (p < 0.01) and an approximately 80% reduction in total B cells (p < 0.05). Broad downregulation of gene signatures associated with T cell and B cell activation, myeloid activation, Type 1 and Type 2 interferon pathways, IL6 production, and innate immune response (p < 0.0001 for all) were observed in RA synovium. The magnitude of reduction of T cell and B cell activation pathways was greater in biopsies from participants treated with rosnilimab that achieved CDAI LDA at Wk 12 compared to non-responders and placebo (Figure. 2).
Conclusions: This Phase 2B rosnilimab study in RA integrates a novel, comprehensive, synovium-focused translational framework that advances understanding of the mode of action and role of pathogenic T cells in disease. Rosnilimab demonstrated on-target activity through selective depletion of pathogenic T cells, key drivers of synovial and systemic inflammation, while preserving regulatory T cell numbers. This was associated with broad modulation of immune pathways and inflammatory mediators in the synovium, supporting the concept that these pathogenic T cells function as upstream mechanistic drivers of RA. Collectively, these findings highlight rosnilimab as a novel therapeutic approach with the potential to address fundamental mechanisms of disease in RA and other autoimmune and inflammatory conditions.
REFERENCES: NIL.
Acknowledgments: NIL.
Disclosure of Interests: Catherine Aversa AnaptysBio, AnaptysBio, Yangsu Ren AnaptysBio, AnaptysBio, Martin Dahl AnaptysBio, AnaptysBio, Eric Hare AnaptysBio, AnaptysBio, Paul Lizzul AnaptysBio, AnaptysBio, Costantino Pitzalis AbbVie, Novartis, Sanofi, Roche/Genentech, UCB, AnaptysBio, AbbVie, Novartis, AbbVie, Novartis, Pfizer, Sanofi, Roche/Genentech, Cailin Sibley AnaptysBio, AnaptysBio.